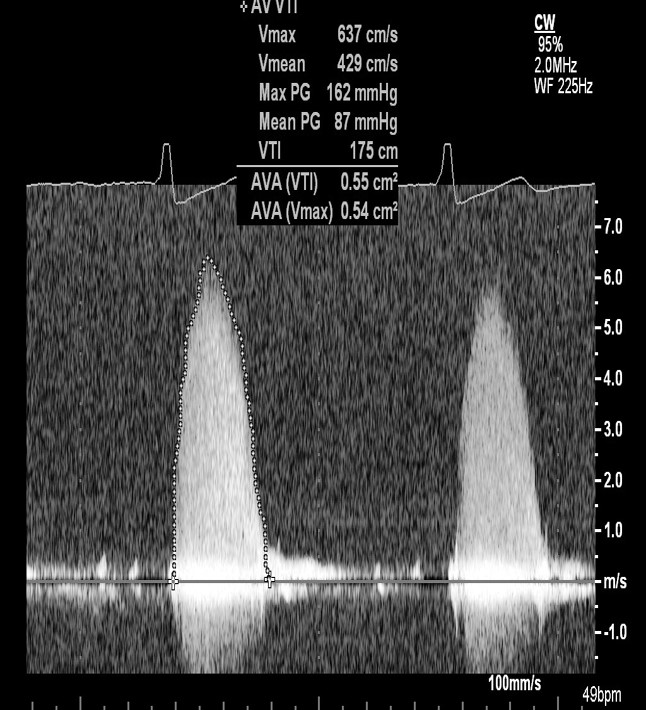
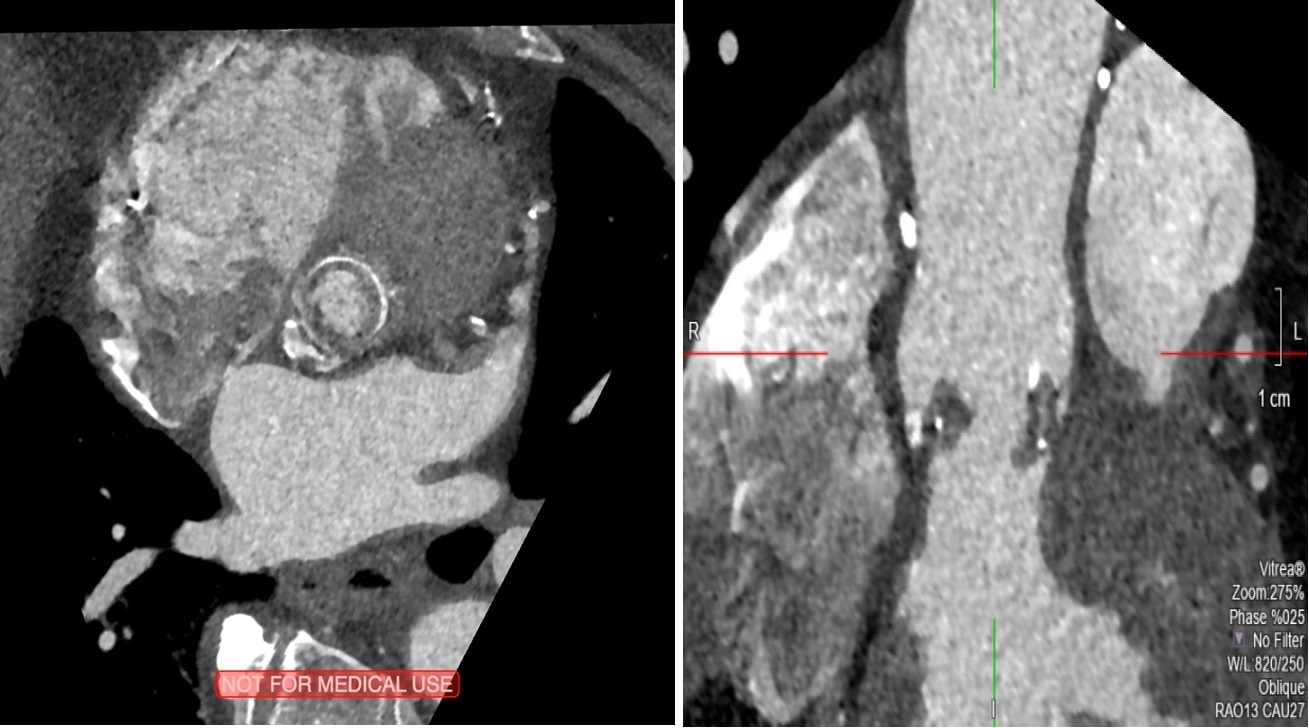
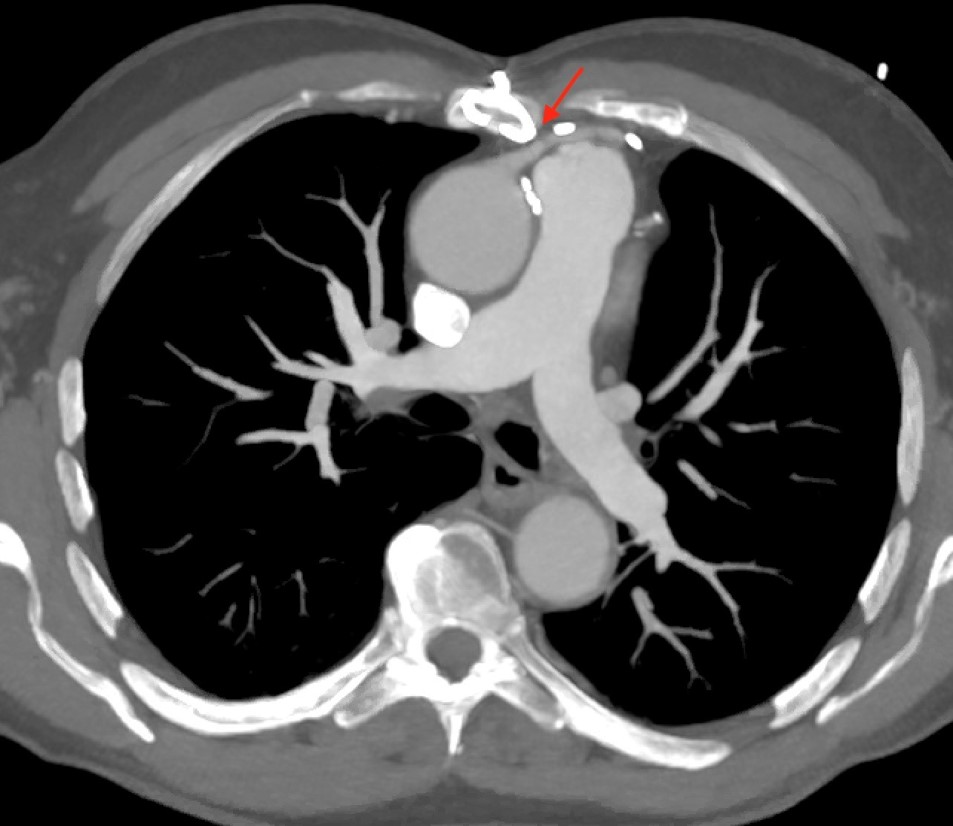
An 82-year-old male patient presented to the echocardiography laboratory for re-evaluation of his aortic valve replacement. The patient has a medical history significant for coronary artery bypass surgery x 3 (left internal mammary artery to the left anterior descending coronary artery [LIMA to LAD], saphenous vein graft to diagonal branch 1 [SVG to Dx1], and saphenous vein graft to posterior descending artery [SVG to PDA]) and bioprosthetic aortic valve replacement in 2006 for severe calcific aortic stenosis. His most recent prior echocardiogram from October 2016, demonstrated moderate prosthetic aortic valve stenosis with a mean transaortic gradient of 34 mmHg and a small anterior paravalvular leak. Other pertinent medical history includes prostate cancer diagnosed in 2004 (treated with chemotherapy and radiation), hypertension, arthritis, and being overweight (body mass index 26.37 kg/m2). The patient is quite active, plays and enjoys senior tennis, works out at the gym, and enjoys long walks. In the last couple of weeks, he has noticed dyspnea on exertion after long walks and had one episode of lightheadedness while walking in New York City, which resolved after a few seconds. Transthoracic echocardiography showed a 23 mm Epic bioprosthetic valve (St Jude Medical, Inc; St Paul, MN) in the aortic position, which appeared to be stable but with leaflet thickening and reduced excursion. A small anterior paravalvular leak was identified, and there was worsening severe prosthetic aortic valve stenosis, with a mean transaortic gradient of 87 mmHg at a heart rate of 55 bpm (Figure 1). Left ventricular and right ventricular size and systolic function were normal without regional variability and an estimated left ventricular ejection fraction of 60%. His electrocardiogram demonstrated sinus bradycardia with first degree atrioventricular block, and voltage criteria for left ventricular hypertrophy. Chest X-ray demonstrated prior median sternotomy with clear lungs bilaterally. Comprehensive metabolic panel, renal function, liver function tests, and complete blood count were all normal. His 30-day Society of Thoracic Surgery-Predicted Risk of Mortality (STS-PROM) score calculated at 2.65%. Cardiac computed tomography (CT) was performed and demonstrated a right and left iliofemoral diameter of 7.1 mm and 7.5 mm, respectively. His bioprosthetic aortic valve was noted to have hypodensities along the leaflets, likely from pannus formation. The measured Hounsfield units were approximately 145 HU (Figure 2). The maximum annulus diameter was 30 mm, and the minimal annulus diameter was 22 mm. These measurements were taken just below the bioprosthetic aortic valve. The mean annulus diameter was 26 mm. The ostial height of the left coronary artery was 15 mm, and the right coronary artery ostial height was 25 mm. His saphenous vein graft was noted to be attached to one of his sternal wires (Figure 3). Coronary angiography demonstrated his LIMA to LAD, SVG to PDA, and SVG to Dx1 were all patent. The patient otherwise was noted to have a 60% stenosis in his native left main and 100% occlusion of his ostial right coronary artery.
Figure 1
Figure 1
Figure 2
Figure 2
Figure 3
Figure 3
What is the best therapeutic option for this patient?
Show Answer
The correct answer is: B. Valve-in-valve transcatheter aortic valve replacement (TAVR)
Since 1997, cardiac surgeons have increasingly used bioprosthetic rather than mechanical valves, and consequently patients are increasingly presenting with failed bioprostheses. Treatment of these patients is a clinical challenge because they are frequently elderly, and redo-SAVR involves significant morbidity and mortality. This patient has severe bioprosthetic aortic valve stenosis that is causing clinical symptoms due to pannus formation 11 years following his initial surgery and meets American College of Cardiology/American Heart Association/ American Society for Echocardiography appropriate use criteria for intervening on the failing bioprosthetic aortic valve. His STS-PROM score of 2.65% places him at low risk for redo-SAVR; however, this patient was noted to have one of his saphenous vein grafts attached to a sternal wire on cardiac CT imaging. This factor caused our heart team to determine that the patient would be at significantly higher risk for complications associated with median sternotomy. The failing valve is a 23 mm Epic bioprosthetic valve, which is a decent-sized valve made of porcine leaflets, with the leaflets sutured inside the stent. The relatively large size of his prosthesis, with height of his left and right coronary ostia >6 mm, and minimal iliofemoral diameters of >6 mm make this patient a suitable candidate for valve-in-valve TAVR. Balloon aortic valvuloplasty would not be appropriate for this patient because it would offer only short-term palliative therapy for his severe symptomatic prosthetic aortic stenosis. Anticoagulation with warfarin would also not be appropriate for this patient, who has evidence of pannus infiltration of his prosthetic aortic valve, based on the Hounsfield Units, appearance, and overall chronicity from his clinical history. Although superimposed tiny thrombi could also be present, the magnitude of the mean gradient across his prosthesis warranted prompt admission to the hospital and definitive treatment. Medical management with beta-blockers and diuretics would likely increase this patient's risk of mortality because patients with severe prosthetic aortic stenosis are very pre-load dependent, and, unfortunately, there aren't currently good medical therapies for treating severe prosthetic aortic stenosis due to pannus infiltration and leaflet degeneration. This patient underwent successful implantation of a 23 mm CoreValve (Medtronic; Dublin, Ireland) valve-in-valve TAVR. Initially, the mean transaortic gradient in the catheterization laboratory was 17 mmHg, which was felt to be too high to leave. Thus, the interventionalist elected to proceed with balloon aortic valvuloplasty to crack the valve and enlarge. Unfortunately, the balloon was noted to rupture during inflation and was not at the tip of the catheter upon removal. The patient required emergent vascular surgery to remove the retained balloon in the left external iliac artery. Despite rupture of the balloon, the CoreValve remained in stable position within the 23 mm Epic valve. After 8 weeks, the patient completely recovered from his procedures, finished a cardiac rehabilitation program, and resumed most of his normal activities, including walking, traveling, and playing tennis. Despite the need to undergo vascular surgery as a complication of his valve-in-valve TAVR, he is grateful that the echocardiography laboratory "blew the whistle that may have saved my life" and to have avoided a complicated redo-SAVR.
References
Aortic Stenosis Writing Group, Bonow RO, Brown AS, Gillam LD, et al. ACC/AATS/AHA/ASE/EACTS/HVS/SCA/SCAI/SCCT/SCMR/STS 2017 Appropriate Use Criteria for the Treatment of Patients With Severe Aortic Stenosis: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, European Association for Cardio-Thoracic Surgery, Heart Valve Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Am Soc Echocardiogr 2018;31:117-47.
Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017;70:252-89.
Bapat V. Technical pitfalls and tips for the valve-in-valve procedure. Ann Cardiothorac Surg 2017;6:541-52.
Moss AJ, Dweck MR, Dreisbach JG, et al. Complementary role of cardiac CT in the assessment of aortic valve replacement dysfunction. Open Heart 2016;3:e000494.