A 60-year-old man presented to the hospital complaining of severe shortness of breath for 2 weeks. His medical history was significant for daily alcohol consumption and occasional marijuana use. After being originally admitted for pneumonia, it was discovered on transthoracic echocardiography that he had severe aortic regurgitation, a dilated left ventricle with ejection fraction of 30-35%, and moderate-to-severe functional mitral regurgitation. His right ventricle (RV) was also noted to be depressed with some tricuspid regurgitation (TR) present that was difficult to quantify due to poor imaging windows. He was taken to the operating room for aortic and mitral valve replacements.
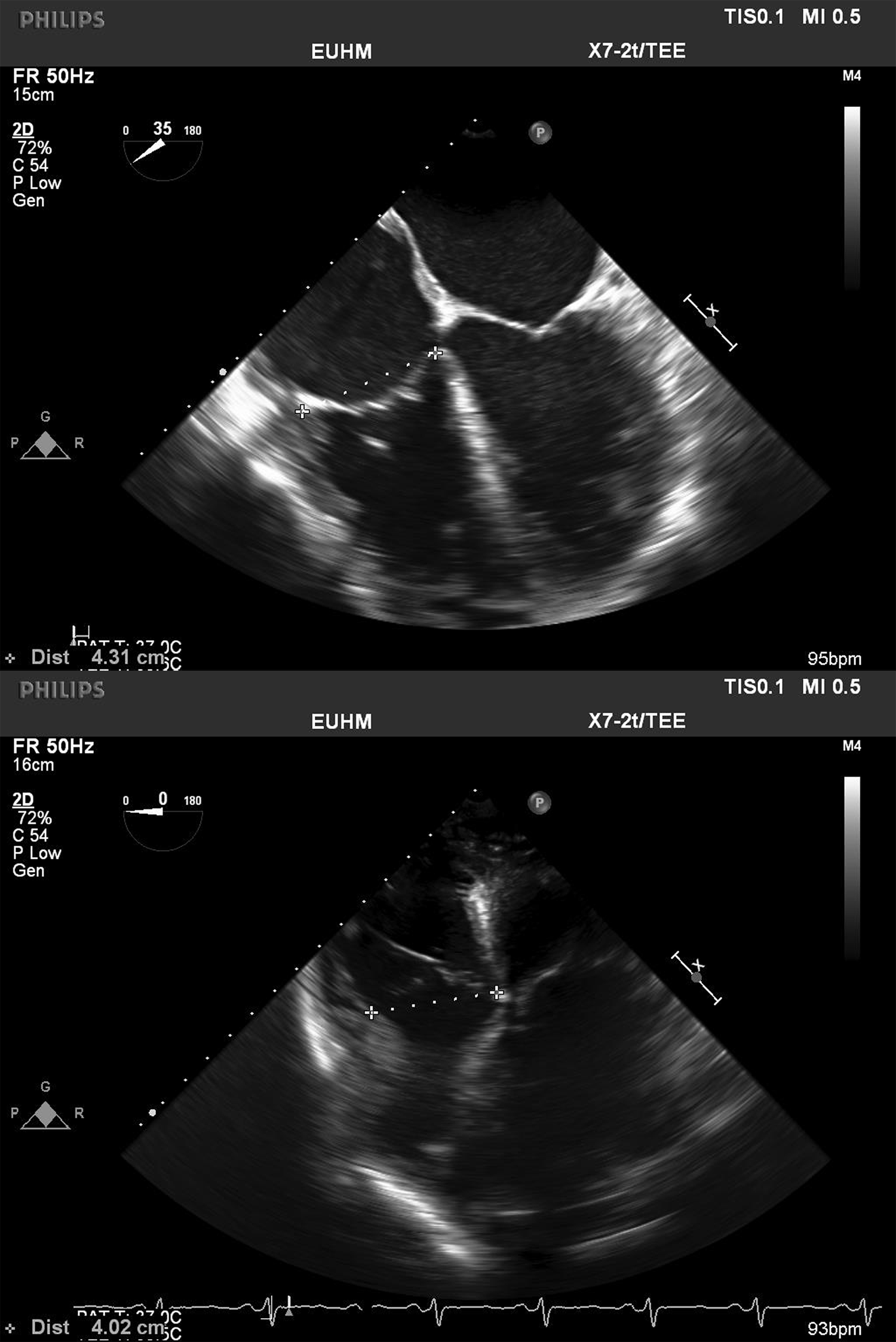
Following induction of anesthesia and placement of invasive monitors, his central venous pressure was noted to be 21 mmHg, and his pulmonary artery pressures were 48/29, with a mean of 37 mmHg. Transesophageal echocardiography (TEE) imaging confirmed the left-sided valvular lesions, as well as a dilated and severely depressed left ventricle (Video 1). The RV was also dilated and moderately depressed (Videos 2-3). The tricuspid valve leaflets appeared tethered (Video 4), resulting in at least moderate TR by color flow Doppler (Videos 5-6). The tricuspid annulus was noted to be dilated, measuring >40 mm in diameter (Figure1).
Video 1
This is a composite video of midesophageal and transgastric TEE images showing a dilated and severely depressed left ventricle, as well as zoomed-in images demonstrating severe aortic and mitral regurgitation by color flow Doppler.
Video 2
Midesophageal four-chamber view on intraoperative TEE.
Video 3
Midesophageal RV inflow-outflow view on intraoperative TEE.
Video 4
Zoomed-in midesophageal four-chamber view on intraoperative TEE.
Video 5
Midesophageal four-chamber view with color flow Doppler across the tricuspid valve on intraoperative TEE.
Video 6
Midesophageal RV inflow-outflow view with color flow Doppler across the tricuspid valve on intraoperative TEE.
Figure 1
Figure 1
Measurement of the tricuspid valve annulus from the midesophageal four-chamber view (top) and modified deep transgastric view (bottom).
Measurement of the tricuspid valve annulus from the midesophageal four-chamber view (top) and modified deep transgastric view (bottom).
In addition to the left-sided valve surgery, what tricuspid valve intervention should be performed?
Show Answer
The correct answer is: C. A tricuspid repair and annuloplasty should be attempted at this time.
Approximately 80% of cases of significant TR are functional in nature and related to tricuspid annular dilation and leaflet tethering in the setting of RV remodeling due to pressure and/or volume overload.1 Although right-heart failure symptoms may be present, patients with severe functional TR may be asymptomatic, making imaging essential. Echocardiography is the modality of choice, although cardiac magnetic resonance imaging may provide more accurate assessment of RV volumes and systolic function, as well as annular dimension and the degree of leaflet tethering (Class IIb, Level of Evidence [LOE] C).2
The 2017 European Society of Cardiology/European Association of Cardiothoracic Surgeons and 2014 American College of Cardiology/American Heart Association guidelines on the management of valvular heart disease recommend that severe functional TR should be addressed during left-sided valve surgery.2,3 It has been demonstrated to provide reverse remodeling of the RV and improvement of functional status (Class I, LOE C).2 In less-than-severe functional TR, the diameter of the tricuspid annulus (rather than the grade of regurgitation) should be the criterion to indicate the need for concomitant TV repair. If the tricuspid annulus is dilated (≥40 mm or ≥21 mm/m2), tricuspid annuloplasty should be performed during left-sided valve surgery (Class IIa, LOE C).2 For patients with mild-to-moderate functional TR undergoing left-sided valve surgery, tricuspid repair may be considered even in the absence of annular dilation when previous recent right-heart failure and/or pulmonary artery hypertension has been documented (Class IIb, LOE C).2,3
Answer A is incorrect because the goal of addressing functional TR during left-sided valve surgery is to decrease the incidence of needing re-operative cardiac surgery for isolated TR, which is associated with a high morbidity and mortality.4 Although there may be temporary improvement in TR severity and RV performance when correcting only the left-sided valve lesions, this benefit is lost within 3 years of the initial operation.5
Answer B is incorrect because, despite poor ventricular function, there is little evidence to suggest adding a tricuspid valve repair to left-sided heart valve surgery increases morbidity or mortality.6 Most tricuspid repairs add only 10-15 minutes of cardiopulmonary bypass time and may even be performed without an aortic cross-clamp, thus limiting ischemic time. Transcatheter interventions are an appealing alternative to surgery for high-risk surgical candidates, and numerous tricuspid transcatheter techniques have been developed to treat functional TR.7 However, at present, most of these clinical experiences have been in compassionate patient cases or small clinical trials. Therefore, limited experimental data have been published, and the potential role for these procedures needs to be determined.
Answer D is incorrect because in cases of severe functional TR, tricuspid replacement has been associated with a higher operative mortality and worse long-term clinical outcomes.8 Trends from the Society of Thoracic Surgeons cardiac surgical database have shown that despite increasing comorbidities, the mortality from tricuspid repair has decreased, and tricuspid valve replacement is associated with increased operative mortality.9 Most valves are amenable to annuloplasty, and the number of repairs performed annually has steadily increased over time.9
References
Martin AK, Mohananey D, Ranka S, Riha H, Núñez-Gil IJ, Ramakrishna H. The 2017 European Society of Cardiology (ESC)/European Association of Cardiothoracic Surgeons (EACTS) Guidelines for Management of Valvular Heart Disease-Highlights and Perioperative Implications. J Cardiothorac Vasc Anesth 2018;May 16:[Epub ahead of print].
Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:e57-185.
Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2017;38:2739-91.
Baumgartner H. The 2017 ESC/EACTS guidelines on the management of valvular heart disease : What is new and what has changed compared to the 2012 guidelines? Wien Klin Wochenschr 2018;130:168-71.
Desai RR, Vargas Abello LM, Klein AL, et al. Tricuspid regurgitation and right ventricular function after mitral valve surgery with or without concomitant tricuspid valve procedure. J Thorac Cardiovasc Surg 2013;146:1126-32.e10.
Zhu TY, Wang JG, Meng X. Does concomitant tricuspid annuloplasty increase perioperative mortality and morbidity when correcting left-sided valve disease? Interact Cardiovasc Thorac Surg 2015;20:114-8.
Hahn RT. State-of-the-Art Review of Echocardiographic Imaging in the Evaluation and Treatment of Functional Tricuspid Regurgitation. Circ Cardiovasc Imaging 2016;9:e005332.
Jang JY, Heo R, Lee S, et al. Comparison of Results of Tricuspid Valve Repair Versus Replacement for Severe Functional Tricuspid Regurgitation. Am J Cardiol 2017;119:905-10.
Kilic A, Saha-Chaudhuri P, Rankin JS, Conte JV. Trends and outcomes of tricuspid valve surgery in North America: an analysis of more than 50,000 patients from the Society of Thoracic Surgeons database. Ann Thorac Surg 2013;96:1546-52.