A 46-year-old woman with metastatic neuroendocrine tumor underwent echocardiography as part of an evaluation prior to multivisceral transplant. It revealed normal left ventricular systolic function, mild pulmonic insufficiency, and a thickened immobile anterior tricuspid leaflet with severe tricuspid regurgitation (TR) (Figure 1). She developed New York Heart Association Class II symptoms, and follow-up echocardiogram 8 months later revealed a reduced systolic function (ejection fraction 39%), continued severe TR, mild pulmonary hypertension, and color flow turbulence across the pulmonic valve with a peak velocity of 2.43 m/s, peak gradient of 24 mmHg, and worsening, moderate pulmonic regurgitation.
Figure 1
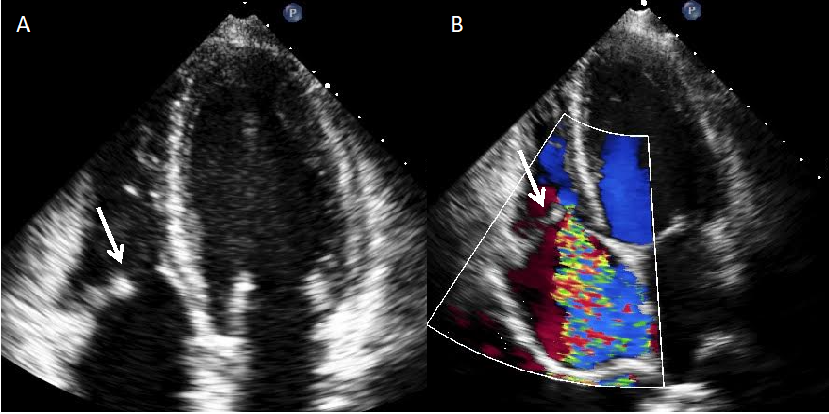
Figure 1
Thickened, immobile anterior tricuspid leaflet (A white arrow) (B white arrow) with severe TR (B).
Thickened, immobile anterior tricuspid leaflet (A white arrow) (B white arrow) with severe TR (B).
What is the best next step in management?
Show Answer
The correct answer is: C. Refer her for tricuspid and pulmonic valve replacement prior to multivisceral transplant.
Carcinoid tumors are rare neuroendocrine malignancies capable of producing metastases. Cardiac manifestations, known as carcinoid heart disease, confer a worse prognosis and are present in up to 20% of patients with carcinoid syndrome.1 Tricuspid disease precedes the pulmonary valve manifestations. Classically, both tricuspid and pulmonary valve leaflets and the corresponding subvalvular apparatus are thickened. Excursion of the leaflets is initially reduced, and following that the leaflets become fixed and non-coapting in a semi-open position, causing functional stenosis and regurgitation.1 Despite some patients having relatively milder pulmonary valve involvement, pulmonary valve replacement in addition to tricuspid valve replacement has been shown to reduce right ventricular size after surgery compared with patients with isolated tricuspid valve replacement.1-3 In our patient, tricuspid and pulmonic valve replacement were recommended, and a 23 mm tissue valve and 25 mm homograft were placed, respectively, with an uneventful recovery.
In conclusion, carcinoid heart disease is a rare complication of neuroendocrine tumors, and it heralds a decline in clinical outcome associated with increased morbidity and mortality. Early recognition and intervention may improve outcomes.