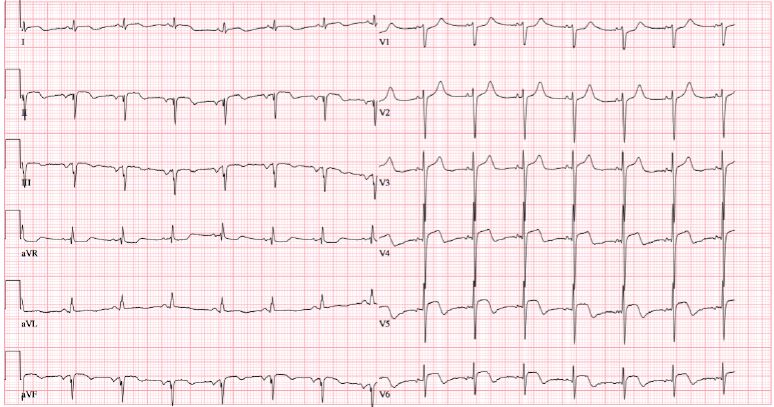
A 49-year-old man presented to the emergency department with a 3-day history of chest pain, flu-like symptoms, and palpitations. His medical history was significant for hypertension, dyslipidemia, diabetes mellitus, and anxiety. On initial examination, he was hypertensive with a blood pressure of 209/137 mmHg and tachycardic with a heart rate of 112 bpm. He was extremely anxious and diaphoretic. The rest of the physical exam was unremarkable. His presenting electrocardiogram (ECG) showed ST-segment elevation in the inferior and antero-lateral leads (Figure 1), consistent with an ST-segment elevation myocardial infarction. Aspirin, clopidogrel, and intravenous unfractionated heparin were administered, and he underwent urgent cardiac catheterization.
Coronary angiography demonstrated only a 40% stenosis in the first obtuse marginal branch with no other evidence of obstructive coronary artery disease (CAD). However, left ventriculography showed apical dyskinesis with normal basal contractility (Video 1). He was transferred to the cardiac intensive care unit for further investigation and management. High-sensitivity Troponin I level from bloodwork drawn on presentation was 3716 ng/L (reference ≤45ng/L), and creatine kinase was 352 U/L (reference 30-250 U/L). Screening for cocaine and amphetamines was negative. A transthoracic echocardiogram (TTE) (Video 2) showed moderate-to-severe left ventricular (LV) dysfunction (LV ejection fraction of 25-35%) and confirmed apical akinesis and normal basal contractility.
Video 1: Left Ventriculogram Showing Normal Basal Contractility and Apical Dyskinesis
Video 2: TTE on Day of Presentation Showing Apical Dyskinesis and Moderately-to-Severely Reduced LV Systolic Function
The next day, he was found to be in circulatory shock (initially presumed cardiogenic) with hypotension; tachycardia; cool, clammy extremities; and decreased urinary output. He was profoundly diaphoretic, drenching the entire bed with sweat. Bloodwork showed an elevated lactate. A pulmonary artery catheter was inserted and showed low central venous pressure (2 mmHg) and low pulmonary capillary wedge pressure (5 mmHg), which was more consistent with hypovolemic shock. He was aggressively fluid resuscitated and quickly recovered clinically and hemodynamically. He was later started on medical therapy for heart failure, including a beta-blocker and an angiotensin-converting enzyme inhibitor.
Cardiac magnetic resonance imaging (MRI) 48 hours later showed that LV function had almost normalized. There was no evidence of late gadolinium enhancement, regional wall motion abnormalities, myocardial edema, or valvular pathology. He was discharged home in stable condition. A repeat echocardiogram 1 week following discharge showed normalized LV function with improved wall motion abnormalities (Video 3).
Video 3: TTE Following Discharge With Normalized LV Systolic Function and Improved Wall Motion Abnormalities
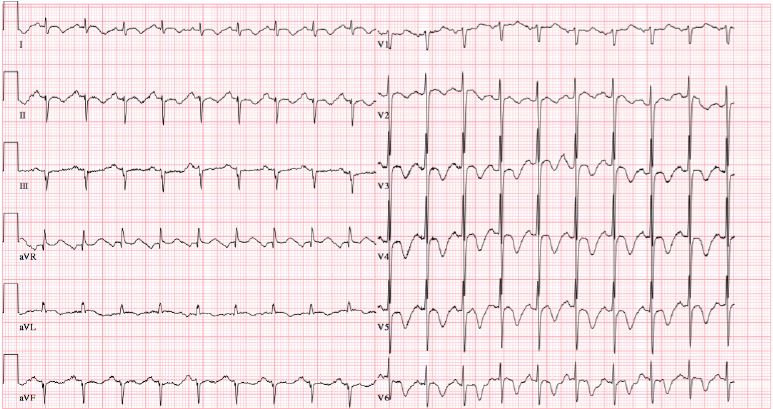
Unfortunately, he presented 2 weeks later with chest pain and was again hypertensive with blood pressure of 190/130 mmHg, tachycardic with a heart rate of 130 bpm, diaphoretic, and extremely anxious. A repeat ECG (which had normalized prior to discharge) demonstrated ischemic changes with deep T-wave inversions in the anterior leads (Figure 2). A repeat echocardiogram showed recurrence of apical akinesis with severe LV dysfunction in a pattern similar to that previously seen. He was admitted to the cardiac intensive care unit; early in his hospital course, he experienced extremely labile blood pressure and paroxysms of tachycardia, diaphoresis, extreme anxiety, and headaches.
Figure 2: ECG on Repeat Presentation
Figure 2
Based on the patient's presentation and angiographic, echocardiographic, and MRI findings, what is the most likely diagnosis?
Show Answer
The correct answer is: B. Recurrent takotsubo syndrome secondary to pheochromocytoma
The history, clinical presentation, and findings on imaging raised strong suspicion for an underlying pheochromocytoma as a secondary cause of recurrent takotsubo syndrome. The 24-hour urine metanephrines were sent, and a computed tomography (CT) scan of the abdomen/pelvis with adrenal protocol was performed. The CT scan (Figure 3) showed a 4.8 cm well-circumscribed, round heterogeneous mass extending from the lateral limb of the right adrenal gland with features consistent with pheochromocytoma. The 24-hour urine metanephrines were greater than 50 times the upper limit of normal of the laboratory reference range (104.3 mmol/d; a normal range is 0.3-2.0 mmol/d), which helped confirm the diagnosis.
Figure 3: CT Scan Showing Right Adrenal Mass
Figure 3
The endocrinology and urology departments were both consulted. The patient was treated with alpha-blockers with gradual reintroduction of beta-blockade as well as aggressive volume expansion with intravenous crystalloid. Screening for multiple endocrine neoplasia syndromes was negative. Two and a half weeks later, he underwent right laparoscopic adrenalectomy. Pathology showed pheochromocytoma with degenerative changes and hemorrhage and negative margins as well as a Pheochromocytoma of the Adrenal Gland Scaled Score of 2 (<4 less likely to be malignant). The patient did very well, with full recovery of LV function on subsequent echocardiography (Video 4).
Video 4: TTE Following Surgery
Takotsubo syndrome is a descriptor of acute and (usually) reversible syndrome LV dysfunction thought to be catecholamine-induced and not due to obstructive CAD. It constitutes about 1-2% of acute coronary syndrome presentations.1 Increasing evidence has shown that it can occur as a consequence of underlying triggers or medical conditions, termed "secondary takotsubo syndrome," such as pheochromocytoma.1,2 Pheochromocytomas are rare catecholamine-secreting tumors in the chromaffin cells of adrenal glands and typically present with paroxysmal episodes of hypertension, headaches, sweating, and tachycardia. Less commonly, they can present with reversible cardiomyopathy.1-5 A recent literature review examined published cases of takotsubo syndrome from 1990 to 2015 and found 80 cases of pheochromocytoma-induced takotsubo compared with 1,750 cases of primary takotsubo syndrome.2 Pheochromocytoma-induced takotsubo was associated with higher rates of life-threatening complications, including cardiogenic shock, pulmonary edema, and severe LV dysfunction.2,3 In addition, the clinical presentation differed: those with pheochromocytoma were more likely to have ST-segment depression rather than ST-segment elevation, more likely to have tachycardia, less likely to have an emotional trigger, and less likely to have chest pain.2 They were also more likely to have lower LV ejection fractions and require inotropic support. Reverse takotsubo (or inverted takotsubo variant), where there is basal hypokinesis and normal apical wall motion, was more common in patients with pheochromocytoma.2,5 There were also higher rates of recurrence compared with primary takotsubo (17.7% vs. 3.3%, respectively).2
Given that untreated pheochromocytoma can increase the risk of life-threatening cardiac complications, screening should be strongly considered in patients with takotsubo syndrome if the history is suggestive and particularly if the patients present without an obvious initial emotional trigger, with dramatic worsening of their general condition, and development of very severe LV dysfunction, pulmonary edema, and cardiogenic or hypovolemic shock.
Here we present a case of a young man with recurrence of takotsubo, prompting further testing that revealed a pheochromocytoma that was treated successfully with alpha-blockade, volume expansion, and adrenalectomy. This case highlights the importance of vigilance for secondary causes of takotsubo syndrome and, in particular, screening for treatable causes such as pheochromocytoma where appropriate.
References
Lyon AR, Bossone E, Schneider B, et al. Current state of knowledge on Takotsubo syndrome: a Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2016;18:8-27.
Y-Hassan S. Recurrent takotsubo syndrome triggered by undiagnosed pheochromocytoma. Int J Cardiol 2015;187:369-71.
Zhang R, Gupta D, Albert SG. Pheochromocytoma as a reversible cause of cardiomyopathy: Analysis and review of the literature. Int J Cardiol 2017;249:319-23.
Gagnon N, Mansour S, Bitton Y, Bourdeau I. TAKOTSUBO-LIKE CARDIOMYOPATHY IN A LARGE COHORT OF PATIENTS WITH PHEOCHROMOCYTOMA AND PARAGANGLIOMA. Endocr Pract 2017;23:1178-92.
Hernández Ramírez JM, Cárdenes León A, Gobind Sakhrani R. Inverted Tako-tsubo Induced by Pheochromocytoma. Rev Esp Cardiol (Engl Ed) 2016;69:1107-9.