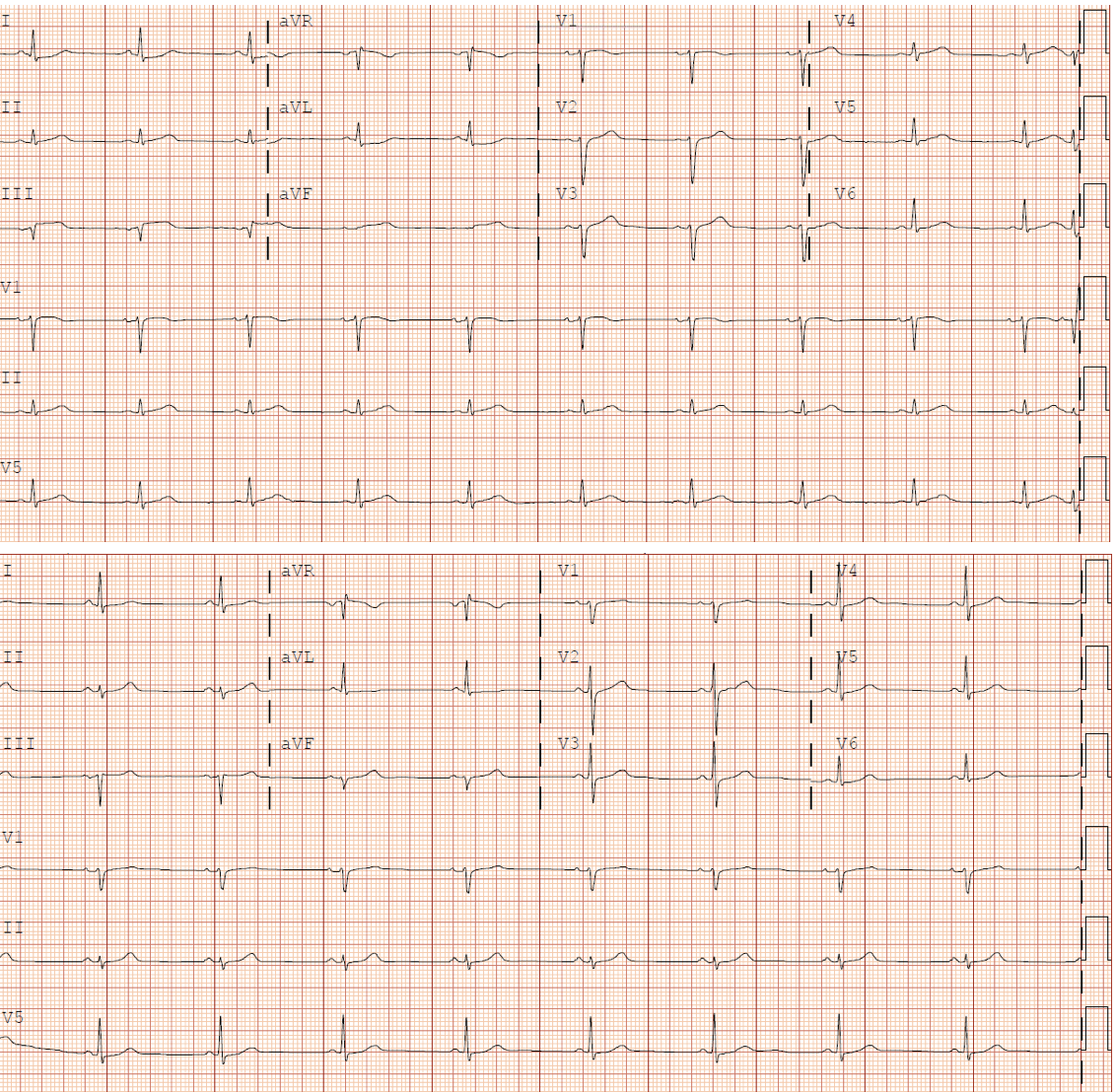
A 45-year-old male patient with recently diagnosed metastatic renal cell carcinoma, status/post right total nephrectomy, left partial nephrectomy, and sternotomy for caval reconstruction and thrombectomy, was admitted for scheduled initiation of high-dose interleukin-2 (IL-2) therapy. He tolerated treatment well, receiving 13 of 14 doses with only mild fevers. On the day of his discharge, he was noted to have a heart rate of 120 bpm but remained largely asymptomatic. The following evening, the patient presented to the emergency department with acute substernal chest pain. Electrocardiography (ECG) revealed ST-segment elevations in the inferior leads (Figure 1). His exam was significant for expiratory wheezes, an S4 gallop, and lower extremity edema. Troponin I was elevated to 73 ng/dL (upper limit of normal <0.8 ng/dL).
Figure 1: 12-Lead ECG With ST-Segment Elevations in Inferior Leads
Figure 1
A baseline ECG is also provided (bottom).
A baseline ECG is also provided (bottom).
What is the most common cardiac complication of IL-2 therapy?
Show Answer
The correct answer is: B. Acute myocarditis
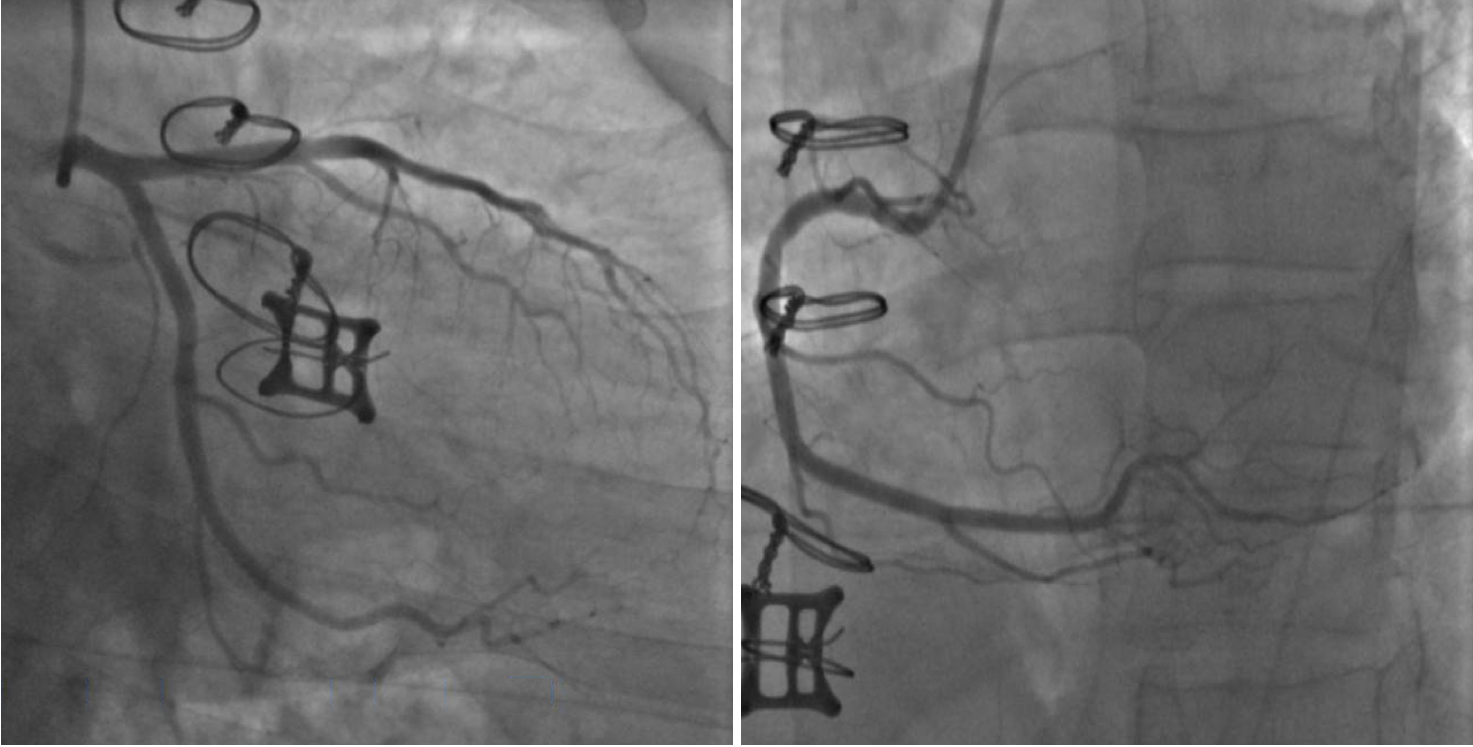
Due to the concern for acute ST-segment elevation myocardial infarction, the patient was sent for emergent coronary angiography that showed no obstructive coronary artery disease and an elevated left ventricular end-diastolic pressure of 25 mmHg (Figure 2). An alternative diagnosis of acute myocarditis was considered, and the patient underwent cardiac magnetic resonance imaging (MRI), demonstrating extensive mid-myocardial and sub-epicardial late gadolinium enhancement (LGE), and T2 weighted imaging, showing diffuse myocardial edema consistent with acute myocarditis (Figure 3). Transthoracic echocardiogram revealed normal left ventricular size and function and no significant valvular abnormalities. The patient was started on low-dose metoprolol tartrate for several non-sustained ventricular tachycardia episodes and intravenous furosemide for capillary leak syndrome (secondary to IL-2 therapy). On the day of discharge, the patient was without chest pain and had returned to a euvolemic status. He has since followed up in cardiology clinic without any complaint of cardiac symptoms.
Figure 2: Coronary Angiography Without Obstructive Disease
Figure 2
Note sternotomy wires from prior caval reconstruction surgery related to the patient's metastatic cancer.
Note sternotomy wires from prior caval reconstruction surgery related to the patient's metastatic cancer.
Figure 3: Cardiac MRI With Extensive Mid-Myocardial and Sub-Epicardial LGE
Figure 3
Although surgical debulking is considered the cornerstone of treatment for renal cell carcinoma, immunotherapy with high-dose IL-2 is a therapeutic option for patients with metastatic disease and good performance status. The side-effect profile of IL-2 mimics that of septic shock through stimulation of pro-inflammatory cytokines (IL-1, tumor necrosis factor-alpha, interferon-gamma), resulting in fever, hypotension, edema, and renal failure (often termed capillary leak syndrome).1 Less commonly, case reports have described the cardiac sequelae of such therapy, most notably acute myocarditis occurring in up to 5% of patients receiving IL-2.2-4 The mechanism of acute myocarditis is not well understood; one proposed hypothesis involves lymphocytic activation and damage to endothelial cells, resulting in cytotoxic injury and cardiomyocyte necrosis.4,5 A diagnosis of acute myocarditis should prompt immediate discontinuation of IL-2. Whether to re-challenge a patient with high-dose IL-2 after an episode of myocarditis is controversial. Recent expert consensus documents support cautious administration of additional cycles of potentially life-saving therapy in patients with full recovery of left ventricular function and resolution of cardiac symptoms.1
This case highlights the use of cardiac MRI for the noninvasive diagnosis of acute myocarditis. In acute myocarditis, necrotic cardiomyocytes are unable to clear gadolinium, leading to characteristic patterns of LGE (sub-epicardial, transmural, and/or patchy enhancement). Although this pattern may also be observed with myocardial fibrosis, T2 weighted imaging will demonstrate increased signal in a similar distribution, supporting a diagnosis of acute myocarditis.4,6
Here we report a case of acute chest pain following high-dose IL-2 therapy, with subsequent diagnosis of acute myocarditis and capillary leak syndrome. The patient was treated with diuresis and beta-blocker therapy and has since been without cardiac symptomology.
References
Dutcher JP, Schwartzentruber DJ, Kaufman HL, et al. High dose interleukin-2 (Aldesleukin) - expert consensus on best management practices-2014. J Immunother Cancer 2014;2:26.
Chow S, Cove-Smith L, Schmitt M, Hawkins R. High-dose interleukin 2-induced myocarditis: can myocardial damage reversibility be assessed by cardiac MRI? J Immunother 2014;37:304-8.
Tan MC, Ortega-Legaspi JM, Cheng SF, Patton KK. Acute myocarditis following high-dose interleukin-2 treatment. J Cardiol Cases 2017;15:28-31.
Thavendiranathan P, Verhaert D, Kendra KL, Raman SV. Fulminant myocarditis owing to high-dose interleukin-2 therapy for metastatic melanoma. Br J Radiol 2011;84:e99-e102.
Zhang J, Yu ZX, Hilbert SL, et al. Cardiotoxicity of human recombinant interleukin-2 in rats. A morphological study. Circulation 1993;87:1340-53.
Dastidar AG, Rodrigues JC, Ahmed N, Baritussio A, Bucciarelli-Ducci C. The Role of Cardiac MRI in Patients with Troponin-Positive Chest Pain and Unobstructed Coronary Arteries. Curr Cardiovasc Imaging Rep 2015;8:28.