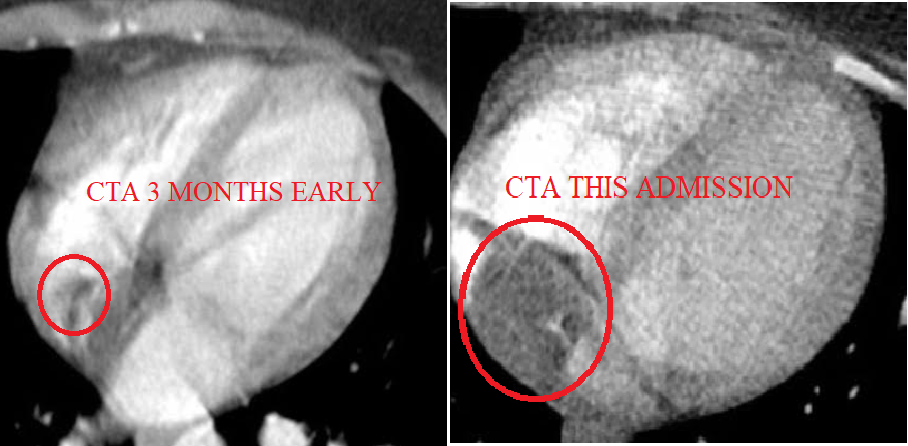
A 21-year-old female patient with a medical history of asthma and multiple presentations to the emergency department with chest pain in the several months prior presented to the emergency department with constant right shoulder pain of 2 days duration. On arrival, she had a blood pressure of 138/71 mmHg, a heart rate of 125 bpm, a respiratory rate of 14/min, a temperature of 100.2°F, and a pulse oximetry of 97% on room air. Except for the patient's tachycardia, both heart and lung examination were unremarkable. During diagnostic workup in the emergency department, thoracic radiography was normal, and an electrocardiogram showed sinus tachycardia. A transthoracic echocardiogram was recommended to evaluate for right heart strain, and it demonstrated a 3 cm mass in the right atrium, mild tricuspid regurgitation, and pulmonary pressures of 50-55 mmHg. A transesophageal echocardiogram (TEE) was then performed, and it showed a 4 x 2.7 cm pedunculated independently mobile mass attached to the high interatrial septum. The mass was heterogeneous with a serpiginous hyperdensity attached to it. The mass did not involve the tricuspid valve annulus or the valve itself. On review of a computed tomography (CT) scan obtained 3 months earlier when the patient presented with similar symptoms, CT then showed a very small mass, indicating that the mass grew to over 3 times its original size in less than 3 months.
Figure 1
The correct answer is: C. Right atrial solid mass with resulting pulmonary embolism (PE)
Right atrial myxoma can predispose patients to embolic events such as PE. Surgery for large myxomas may be necessary to reduce the risk of PE. Three-dimensional TEE is typically a sufficient technique for the diagnosis and evaluation of shape, size, origin, and hemodynamic consequences of cardiac masses and to serve as a guide for surgical treatment. Surgery is also an important modality for preventing further venous thromboembolism after a first event. Treatment for this patient's PE started with conventional therapy using heparin and was bridged to warfarin. She was ultimately scheduled for surgical intervention, although this did not occur due to the patient's noncompliance with subsequent visits. Thrombolysis as an initial therapy may be indicated as an alternative strategy if there is hemodynamic compromise or right ventricular strain due to the PE.
References
- Kalvakuri K, Banga S, Upalakalin N, Shaw C, Davila WF, Mungee S. Metastatic right ventricular mass with intracavitary obliteration. J Community Hosp Intern Med Perspect 2016;6:31679.
- Diaz A, Di Salvo C, Lawrence D, Hayward M. Left atrial and right ventricular myxoma: an uncommon presentation of a rare tumour. Interact Cardiovasc Thorac Surg 2011;12:622-3.
- Jara-Palomares L, Serrano-Gotarredona MP, Lopez-Haldón J, et al. Right atrium mass in a 28-year-old patient with pulmonary embolism taking contraceptives. J Atheroscler Thromb 2011;18:829-32.
- Kasper DL, Fauci A, Hauser S, Longo D, Jameson JL, Loscalzo J. Harrison's Principles of Internal Medicine. 19th ed. New York: McGraw-Hill; 2015.
- Aydın C, Taşal A, Ay Y, Vatankulu MA, Inan B, Bacaksız A. A giant right atrial villous myxoma with simultaneous pulmonary embolism. Int J Surg Case Rep 2014;5:206-8.
- Abela OG, Diep J, Mavroidis D. RIGHT ATRIAL MASS AND PULMONARY EMBOLISM: WHO WAS HERE FIRST? J Am Coll Cardiol 2015;65:Issue 10 Supplement.