A 22-year-old man with a medical history of stage IV neuroblastoma, diagnosed at the age of 3, is noted to have a cardiac mass. Prior cancer-directed therapy included surgical resection, chemotherapy with 150 mg/m2 cumulative dose of doxorubicin, etoposide, high-dose alkylating agents, cisplatin, and carboplatin; total body irradiation; and autologous bone marrow transplant. Post-therapy, he did not relapse but developed late effects from cancer-directed therapy. He has growth hormone deficiency, primary hypothyroidism, primary hypogonadism, and osteochondroma of the wrist.
At long-term follow-up, a screening transthoracic echocardiogram (TTE) noted a single, echodense, well-circumscribed, globular, 1.3 x 1.0 cm mass in the anterolateral aspect of the mid to apical portion of the left ventricle (LV) (Figure 1). On three-dimensional (3D) TTE, the mass appeared pedunculated and predominantly homogenous with some echolucent areas (Figure 2). There was normal biventricular and valvular function and no pericardial effusion. Cardiac magnetic resonance imaging (MRI) demonstrated a T2 hyperintense mass located near the anteroseptal wall of the LV and attached to the anterior wall by thin septae (Figure 3A). The mass was slightly mobile with each cardiac cycle without evidence of outflow or inflow obstruction. There was no clear enhancement on the first pass perfusion imaging and the 1-minute delayed imaging; however, delayed gadolinium enhancement was present on the 10-minute post-contrast delayed imaging (Figure 3B-C).
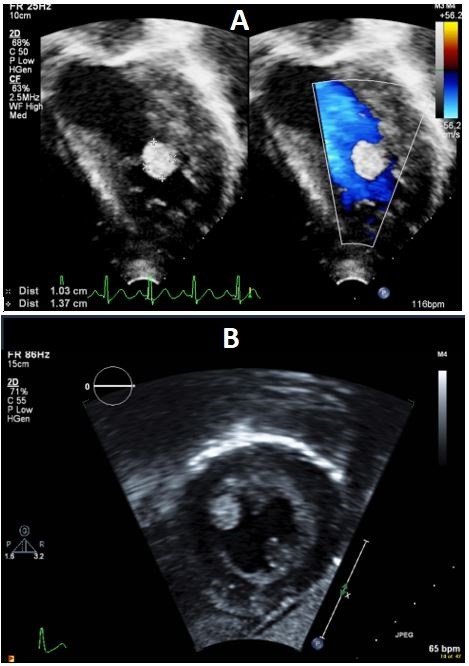
Figure 1
Figure 1
(A) Apical four-chambers view with color compare. (B) Subcostal short-axis view, showing a single mass attached to the anterolateral aspect of the mid to apical portion of the LV.
(A) Apical four-chambers view with color compare. (B) Subcostal short-axis view, showing a single mass attached to the anterolateral aspect of the mid to apical portion of the LV.
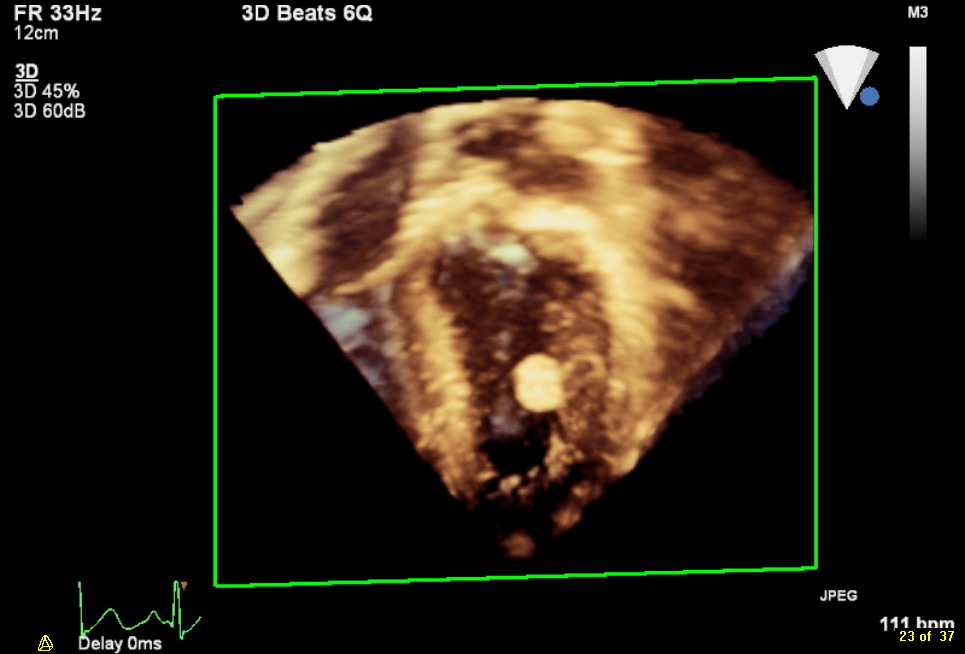
Figure 2
Figure 2
3D TTE, apical four-chambers view with a single, pedunculated, almost homogenous mass.
3D TTE, apical four-chambers view with a single, pedunculated, almost homogenous mass.
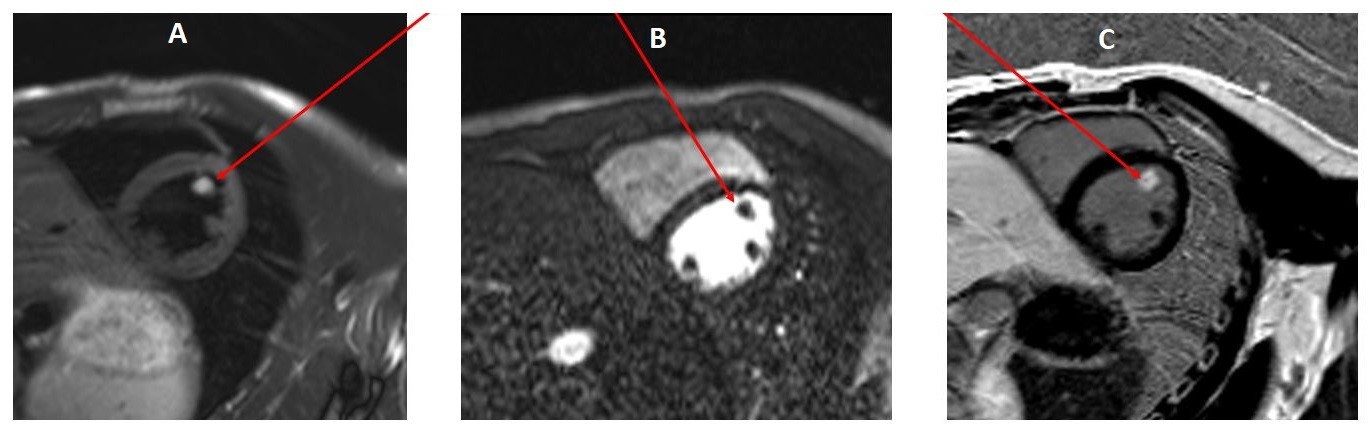
Figure 3
Figure 3
Cardiac MRI images of the mass for tissue characterization. (A) T2-weighted image with fat suppression. (B) First-pass perfusion after Gadolinium infusion. (C) 10-minutes delayed Gadolinium enhancement.
Cardiac MRI images of the mass for tissue characterization. (A) T2-weighted image with fat suppression. (B) First-pass perfusion after Gadolinium infusion. (C) 10-minutes delayed Gadolinium enhancement.
Taking into consideration the clinical presentation and cardiac imaging findings, what is the likely etiology of the mass?
Show Answer
The correct answer is: D. Papillary fibroelastoma (PFE)
The diagnosis of a cardiac mass can often be a challenge. Careful assessment of a patient's clinical history along with the echocardiographic and other advanced imaging (cardiac MRI) characteristics can narrow the differential diagnosis.
Even though cardiac involvement by secondary malignancies is more frequent (by 20-40 times) than primary cardiac tumors,1 cardiac metastasis from neuroblastoma is extremely rare. There is a single case report in which metastatic involvement of the LV by neuroblastoma was described.1 The proposed mechanisms for cardiac metastasis from a neuroblastoma included micro-dissemination through hematogenous pathway, direct extension, or lymphatic spread.1 With those mechanisms in mind, it would be extremely unlikely for a cardiac metastasis to develop after 12 years of cancer-free survival and with no other signs of recurrent tumor. A cardiac metastasis is traditionally visualized as an irregular mass with or without pericardial effusion,2 neither of which was present in our patient's case. Our patient's cardiac mass lacked the characteristic MRI feature of a cardiac lipoma, which would be hyperintense on T1- and T2-weighted images and with decreased signal on fat-saturated images.2
A thrombus was also unlikely, given the normal LV function and normal sinus rhythm. On cardiac MRI, acute thrombus is hyperintense on both T1-and T2-weighted images, and chronic thrombus is hypointense on both T1- and T2-weighted images. The signal characteristics of this mass did not match acute or chronic thrombus. Angiosarcomas are typically located in the right atrioventricular groove, with frequent involvement of the pericardium and right atrial wall.3 On cardiac MRI, angiosarcoma appears as a heterogeneous, nodular mass in the right atrium, and, grossly, there are invariably areas of hemorrhage.3
Because of the MRI characteristics of the mass, the mass was thought to be a benign tumor, specifically PFE or myxoma. Because of the potential risk for systemic embolization given the location and shape of the lesion, the decision was made for surgical removal of the mass. On gross specimen, the mass was pink-gray colored, rubbery, cystic, and contained gelatinous material. Microscopic evaluation confirmed the diagnosis of PFE.
PFE and cardiac myxoma are the most common benign tumors of the heart, and a recent report suggests that PFE is more frequent than cardiac myxoma. Unlike myxomas, which are most commonly located in the left atrium,3 PFEs are typically found on the valvular surfaces of the heart. Non-valvular PFEs are exceedingly rare, most commonly located in the LV.4,6 Despite their benign nature, cardiac PFEs can rarely cause potentially life-threatening complications, such as peripheral or coronary embolization.7-9
3D echocardiography can provide accurate information on mass size, position, and attachment. Cardiac MRI is excellent for mass characterization and evaluation of myocardial infiltration. Almost all cases of PFEs are sporadic. However, a few case reports have described an association between neuroblastoma and other tumors like myxomas10 and secondary cardiac metastasis.1 This is the first report of a PFE in the context of neuroblastoma. Our patient received total-body irradiation, and although radiation has been associated with cardiac fibrosis and cardiovascular disease, a literature review did not confirm an association with benign cardiac tumors.
The reported case highlights the role of screening echocardiograms for cancer survivors who have received supra-diaphragmatic radiation and/or anthracyclines and raises the question of a relationship among radiation, chemotherapy, prolonged immunosuppression, and nonmalignant cardiac tumors.
References
Gupta D, Srikanthan M, Lagmay J, Co-Vu JG. Left Ventricular Metastasis in Neuroblastoma: A Case Report. J Pediatr Hematol Oncol 2016;38:74-7.
Sparrow PJ, Kurian JB, Jones TR, Sivananthan MU. MR imaging of cardiac tumors. Radiographics 2005;25:1255-76.
Burke A, Tavora F. The 2015 WHO Classification of Tumors of the Heart and Pericardium. J Thorac Oncol 2016;11:441-52.
Tamin SS, Maleszewski JJ, Scott CG, et al. Prognostic and Bioepidemiologic Implications of Papillary Fibroelastomas. J Am Coll Cardiol 2015;65:2420-9.
Gowda RM, Khan IA, Nair CK, Mehta NJ, Vasavada BC, Sacchi TJ. Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases. Am Heart J 2003;146:404-10.
Nomoto N, Tani T, Konda T, et al. Primary and metastatic cardiac tumors: echocardiographic diagnosis, treatment and prognosis in a 15-years single center study. J Cardiothorac Surg 2017;12:103.
Rosenfield K, Ghoshhajra BB, Dudzinski DM, Stone JR. CASE RECORDS of the MASSACHUSETTS GENERAL HOSPITAL. Case 9-2016. A 29-Year-Old Man with Dyspnea and Chest Pain. N Engl J Med 2016;374:1178–88.
Antonopoulos AS, Chrysohoou C, Lymperiadis D, Brili S, Tousoulis D. Peripheral and coronary artery embolisms due to left ventricle fibroelastoma. Hellenic J Cardiol 2016;57:368-70.
Zamolo F, Calvagna C, D'Oria M, Sgorlon G, Zandonà L, Adovasio R. Neoplastic Embolization from Cardiac Papillary Fibroelastoma with Unusual Presentation: A Case Report. Ann Vasc Surg 2017;38:317.e1-317.e4
Hill G, Castellino S, Williams D. Cardiac myxoma after treatment for childhood neuroblastoma. Pediatr Cardiol 2009;30:340-2.