A 27-year-old woman with history of methamphetamine abuse and hepatitis C developed acute hypoxemia 2 days after a cesarean section (performed for intrauterine growth retardation). Physical exam revealed a loud P2, pan-systolic murmur at the left lower sternal border and a right parasternal heave. Vitals were notable for SpO2 of 78-85% on a non-rebreather. A chest computed tomography scan showed no pulmonary embolism or parenchymal lung disease. Transthoracic echocardiogram revealed an under-filled left ventricle (LV), a severely dilated and dysfunctional right ventricle (RV), severe tricuspid regurgitation (TR), an estimated RV systolic pressure of 100-105 mmHg, and a small (1 cm) secundum atrial septal defect (ASD) with predominantly right-to-left shunt (Figure 1).
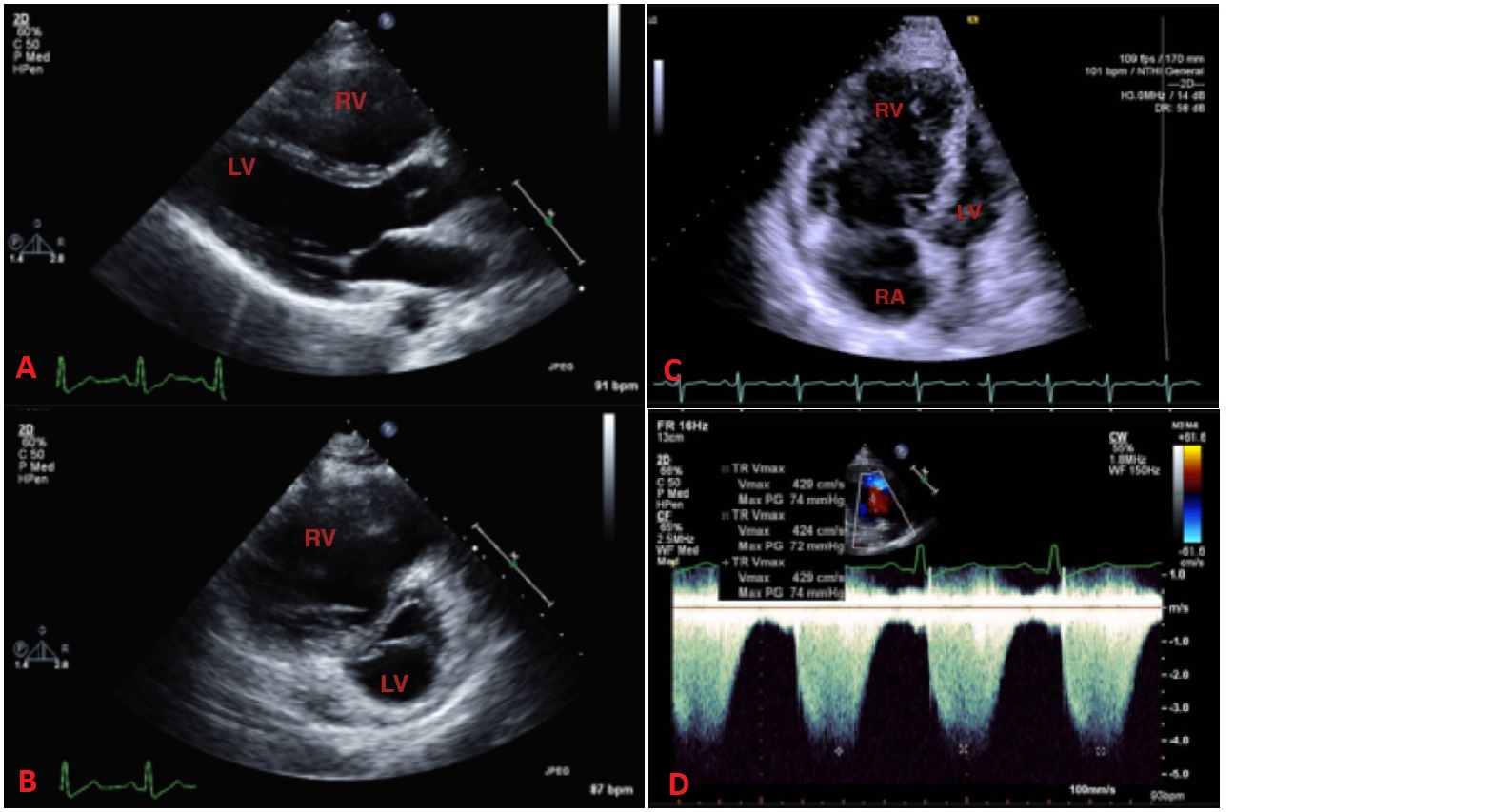
Figure 1: Transthoracic Echocardiogram
Figure 1
(A: parasternal long-axis view) Grossly dilated RV. (B: parasternal short-axis view) Severely enlarged RV with septal flattening and a small, compressed LV. (C: apical four-chamber view) Severely enlarged right atrium and RV, again with septal flattening and a small, compressed LV. (D: Color Doppler across tricuspid valve) Regurgitant tricuspid valve jet of 4.3 m/s, with an estimated RV systolic pressure of approximately 90 mmHg, which is severely elevated and indicates pulmonary hypertension.
(A: parasternal long-axis view) Grossly dilated RV. (B: parasternal short-axis view) Severely enlarged RV with septal flattening and a small, compressed LV. (C: apical four-chamber view) Severely enlarged right atrium and RV, again with septal flattening and a small, compressed LV. (D: Color Doppler across tricuspid valve) Regurgitant tricuspid valve jet of 4.3 m/s, with an estimated RV systolic pressure of approximately 90 mmHg, which is severely elevated and indicates pulmonary hypertension.
A right heart catheterization showed the following:
Pulmonary artery (PA) saturation: 48%
Superior vena cava saturation: 51%
Inferior vena cava saturation: 53%
Pulmonary veins (PV) (right middle and left upper) saturation: 99%
PA pressure (systolic/diastolic/mean): 105/40/63 mmHg
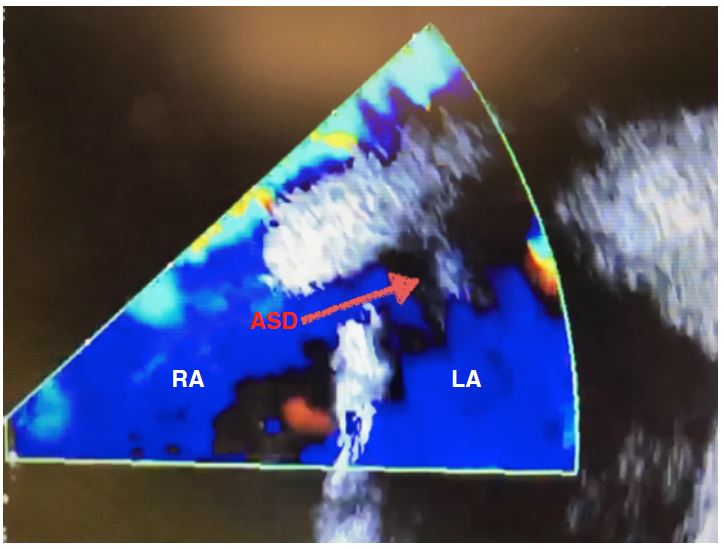
Intracardiac echocardiography confirmed a small secundum ASD with right-to-left shunting (Figure 2).
Figure 2: Intracardiac Echocardiography
Figure 2
Secundum ASD with right-to-left shunting.
Secundum ASD with right-to-left shunting.
Which of the following is the best initial step in management of this patient?
Show Answer
The correct answer is: A. Initiate intravenous pulmonary vasodilators
Based on right heart catheterization numbers that show a mean PA pressure of 63 mmHg, PVR >15.9 Wood units, and PCWP <9 mmHg, our patient has severe pulmonary arterial hypertension (PAH), by definition. Because the patient had acute, severe, symptomatic hypoxemia associated with RV dysfunction on echocardiogram, she should be started on intravenous pulmonary vasodilator therapy as soon as possible. Based on 2018 American College of Cardiology and American Heart Association adult congenital heart disease (CHD) guidelines, severe PAH is a contraindication to ASD closure, and its presence must be accurately excluded prior to considering closure. ASD closure should not be performed in adults with PA systolic pressure greater than two-thirds systemic, PVR greater than two-thirds systemic, or those with right-to-left shunt. PAH is frequently encountered in female patients, and the first clinical manifestations may be seen in pregnancy. After 2 weeks of therapy with aggressive titration, our patient was weaned off of supplemental oxygen, and shunt flow reversed to left-to-right on a repeat echocardiogram.
Answers B and C are incorrect; it is contraindicated to close the ASD in this case due to presence of severe PAH and right-to-left shunt, whether it be done through a transcatheter or surgical procedure. To evaluate the patient with PAH and ASD for closure of defect, it is important to ensure that the shunt remains left to right, despite elevated PVR and/or pulmonary pressure, and that pulmonary pressure and PVR are accurately measured. Because of the complexity of PAH in the setting of CHD, these cases are best evaluated in collaboration with an adult CHD cardiologist and a pulmonary hypertension expert provider to develop the most appropriate management plan. In our case, initiating pulmonary vasodilator therapy is the best initial step to treat severe PAH. Once severe PAH is treated, and a significant left-to-right shunt is demonstrable after treatment with PAH therapies, closure of an ASD can then be considered if other indications are met. Pretreatment with PAH therapies and PA remodeling agents, with a demonstrated reduction in PA resistance of >20%, portends a favorable prognosis after ASD closure. Although left-to-right shunting was the initial research model of triggered PAH, pulmonary hypertension in patients with CHD including ASD (like in this case) can be caused by or associated with pulmonary venous hypertension (post-capillary), parenchymal or restrictive lung disease, thromboembolic disease, portal hypertension, or toxin exposure.
Answer D is incorrect; there is no indication to replace the tricuspid valve. The patient has functional severe TR, secondary to RV enlargement and dysfunction. There is no inherent problem with the valve, just annular dilation leading to regurgitation. Correction of the RV dysfunction with administration of pulmonary vasodilators will most likely significantly reduce the severity of TR.
References
Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC Guideline for the Man-agement of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guide-lines. J Am Coll Cardiol 2018;Aug 10:[Epub ahead of print].
Opotowsky AR. Clinical evaluation and management of pulmonary hypertension in the adult with congenital heart disease. Circulation 2015;131:200-10.
Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J 2018:39:3165-241.