Pancreatic Cancer Presenting as Recurrent Endocarditis
A 74-year-old Caucasian female with a history of paroxysmal atrial fibrillation on apixaban, hypertension, and recent transient ischemic attack presented to the emergency department with palpitation, nausea and diarrhea, epigastric discomfort, and generalized fatigue. She denied any chest pain, shortness of breath, leg swelling, orthopnea, or syncope. The patient was hemodynamically stable at the time of initial presentation. Her physical exam was significant for diastolic murmur in the left second intercostal space. Her initial laboratory results follow:
- Hb = 13.6
- Platelets = 85,000
- White blood cell count = 5.5
- Creatinine = 0.85
- Troponin = 0.13
- Erythrocyte sedimentation rate = 13
- Blood cultures were negative
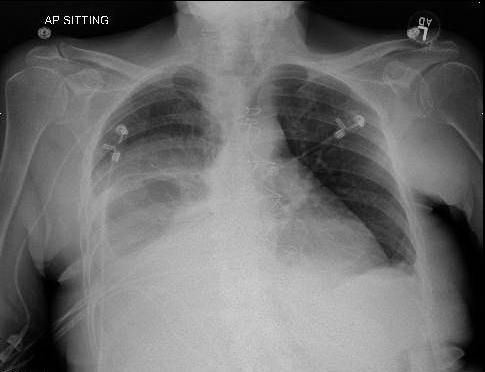
A transthoracic echocardiogram showed mobile echodensity (1.96 x 0.47 cm) attached to the right leaflet of aortic valve projecting the left ventricular outflow tract as well as a mobile echodensity on the anterior mitral valve leaflet. A subsequent transesophageal echocardiogram showed echodensities on all three leaflets of the aortic valve, the largest being 2.2 x 0.5 cm. She was empirically started on intravenous ceftriaxone and vancomycin. The patient soon underwent replacement of the aortic valve with #23 bovine bioprosthetic valve (mean gradient = 13 mmHg; peak gradient = 24.6 mmHg; maximum velocity = 2.48 m/s). The post-operative cultures from the aortic valve showed no evidence of bacterial or fungal growth after 4 days of incubation. The patient was subsequently discharged home in a stable condition on intravenous antibiotics as well as anticoagulation but was readmitted within 2 weeks following hospital discharge with worsening shortness of breath, pedal edema, poor appetite, and generalized fatigue. Her physical exam was significant for elevated jugular venous distention, bilateral lower extremity edema, and grade 4/6 systolic murmur best heard in the second left intercostal space. Her initial electrocardiogram and chest X-ray are shown in Figures 1-2.
Figure 1
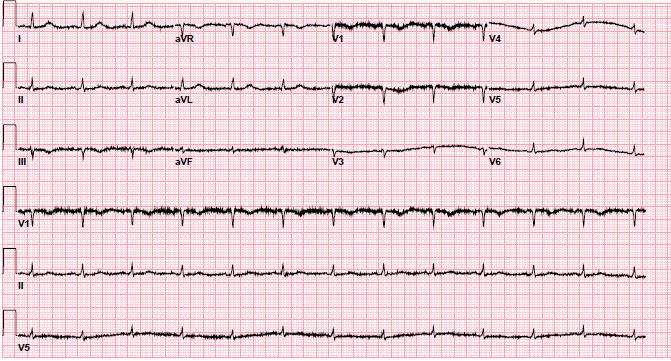
Figure 2
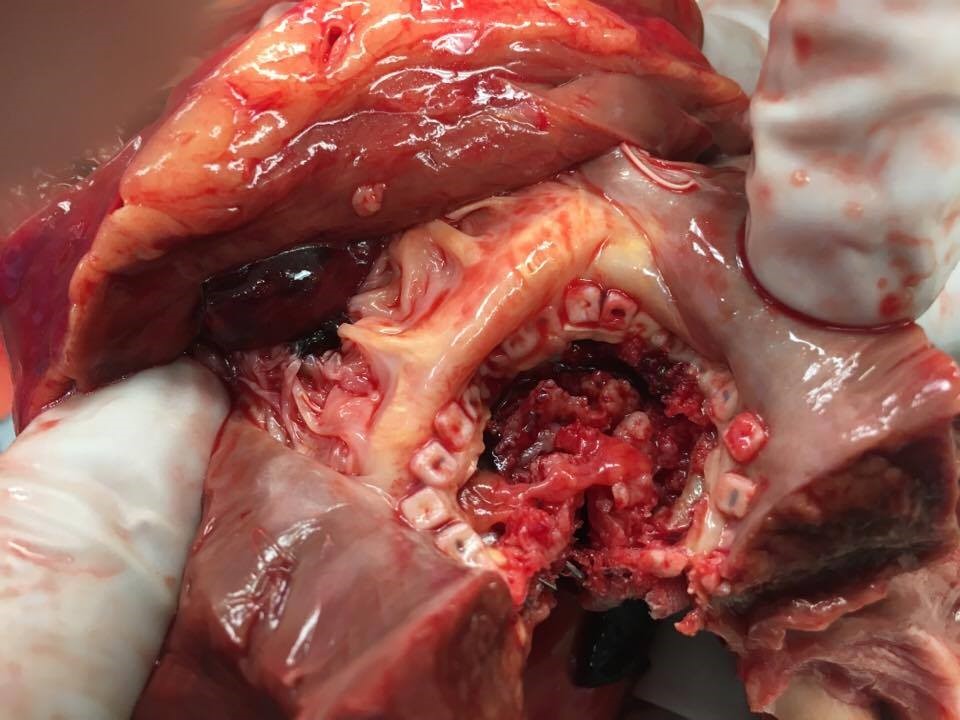
A repeat echocardiogram showed a large pericardial effusion with evidence of tamponade and #23 bovine bioprosthetic aortic valve with elevated gradients (mean gradient = 53 mmHg; peak gradient = 77 mmHg; maximum velocity = 4.5 m/s). She was immediately taken for a pericardial window, but she sustained cardiac arrest during the procedure and could not be resuscitated. Pericardial fluid was positive for malignant cells consistent with metastatic adenocarcinoma. An autopsy showed evidence of stage 4 pancreatic cancer (Figures 3-4).
Figure 3
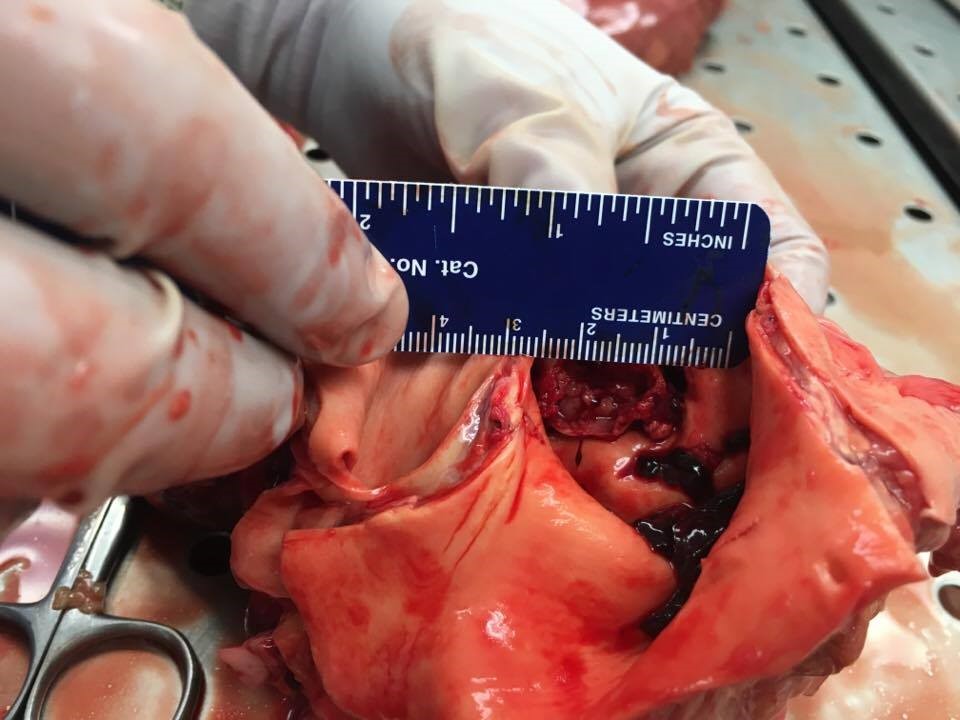
Figure 4
What is this patient's diagnosis?
Show Answer