A 74-year-old female patient with a history of breast cancer, aortic valve stenosis, type II diabetes mellitus, and hypothyroidism was referred to our institution for further evaluation of dyspnea and fatigue. She described progressively worsening dyspnea on exertion, which limited her to a few steps and required her to use a wheelchair at all times. Approximately 6 months prior to her current presentation, she was diagnosed with breast cancer, metastatic to the axial and appendicular spine. She was initiated on everolimus and exemestane along with opioids for pain management. During her current visit, a physical exam demonstrated an oxygen saturation of 84% on room air that improved to 95% with 2L nasal cannula, a soft S1 and a late peaking IV/VI systolic murmur heard best at the right upper sternal border without an A2, no lower extremity edema, and a normal jugular venous pressure. Mild diffuse mid- to end-inspiratory crackles were heard over all lung fields. Her laboratory results were notable for the following:
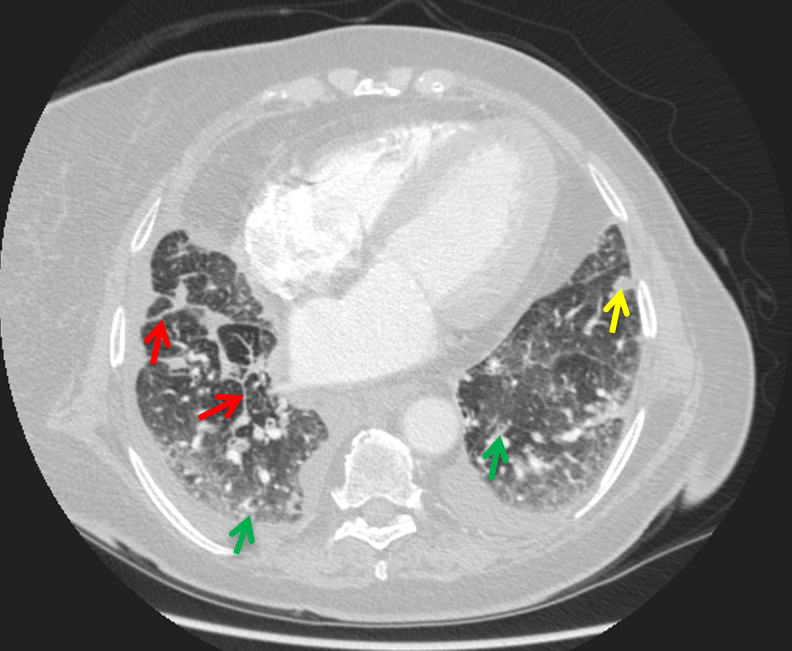
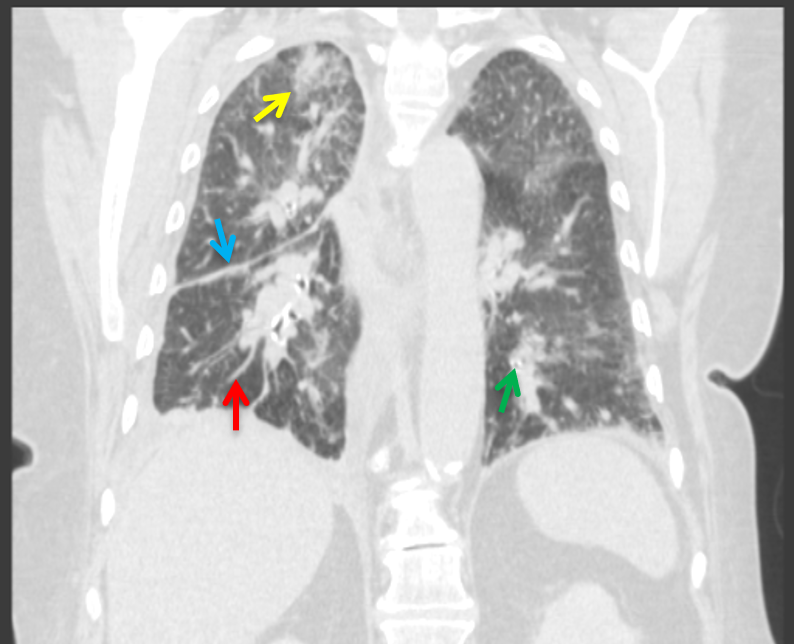
A transthoracic echocardiogram demonstrated an aortic valve area of 0.65 cm2, mean gradient of 49 mmHg, and peak velocity of 4.4 m/s along with an ejection fraction of 53%. A computed tomography (CT) angiogram of the chest (Figures 1-2) was negative for pulmonary emboli but demonstrated interlobular septal thickening (red arrows), scattered nodular consolidative opacities (yellow arrows), bronchial wall thickening (green arrows), bilateral pleural effusions, and nodular changes of the right major fissure (blue arrow). Other findings included enlarged mediastinal and paratracheal lymph nodes.
Figure 1: CT Angiogram of the Chest in Transverse View at Presentation
Figure 1
Figure 2: CT Angiogram of the Chest in Coronal View at Presentation
Figure 2
Based on the clinical presentation, physical exam, and imaging findings, what is the next best step to improve this patient's dyspnea?
Show Answer
The correct answer is: D. Discontinue everolimus and initiate corticosteroids
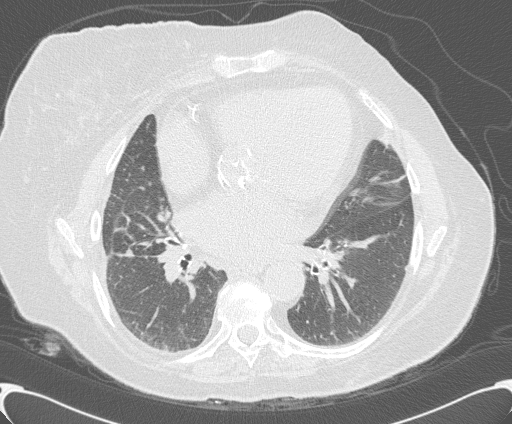
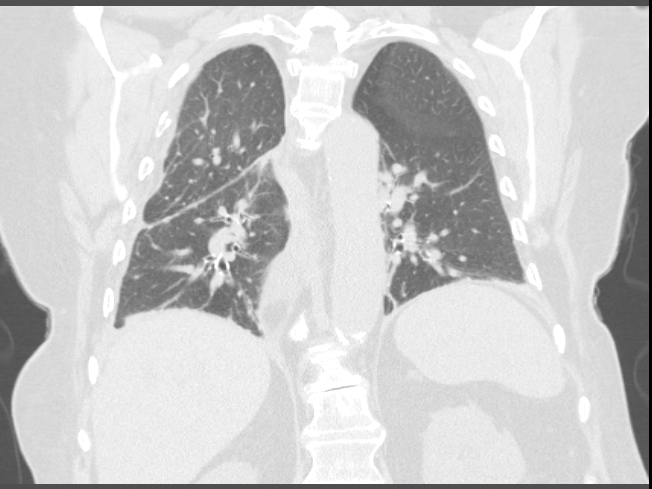
Based on the timing of the patient's symptoms, her euvolemic exam, and CT chest findings, the cause of her subacute worsening of dyspnea is most likely due to everolimus-induced non-infectious pneumonitis. Therefore, her everolimus was discontinued and she was initiated on oral prednisone. Her dyspnea improved within a couple months, and she was weaned off supplemental oxygen. A repeat CT chest performed 2 months after treatment demonstrated near-complete resolution of the patchy consolidative opacities, interlobular and bronchial wall thickening, and pleural effusions, with reduction in size of the mediastinal lymph nodes (Figures 3-4).
Figure 3: CT of the Chest in Transverse View 2 Months After Discontinuing Everolimus and Initiating Corticosteroids
Figure 3
Figure 4: CT of the Chest in Coronal View 2 Months After Discontinuing Everolimus and Initiating Corticosteroids
Figure 4
Everolimus belongs to the mammalian target of rapamycin (mTOR) class of medications, which also includes sirolimus and temsirolimus.1 Use of the mTOR class of medications is growing given its efficacy as a potent immunosuppressant in solid organ transplant and as a chemotherapeutic drug.1,2 Pneumonitis is thought to be a rare side effect of the mTOR inhibitors; however, large series in transplant recipients demonstrate an incidence of up to 15% with an unknown mechanism of injury.2,3 The clinical presentation is often vague and can be variable, including shortness of breath at rest, dyspnea on exertion, fatigue, or respiratory failure.4 Common CT chest imaging findings include inter/intralobular septal thickening, peribronchovascular opacities, and bilateral scattered parenchymal lung consolidations.2-4 Management includes immediate discontinuation of the offending agent, which was everolimus in this case, and corticosteroids should be considered depending on the patient's respiratory status.5,6
The clinician must maintain a high degree of suspicion for non-infectious pneumonitis when patients present with dyspnea and have associated imaging findings while on an mTOR inhibitor. It was particularly important to expand the differential diagnosis in this case because the patient had multiple potential reasons for her dyspnea, including severe aortic valve stenosis and progressive metastatic cancer. Aortic valve replacement or aortic valvuloplasty would not be indicated initially because her imaging findings were concerning for new pulmonary metastases, which would confer a poor prognosis.7 Additionally, she did not have signs or symptoms of infection; therefore, antibiotics should not be initiated.
Given that the patient improved dramatically after treatment of her everolimus-induced pneumonitis, her prognosis was believed to be more favorable. She ultimately underwent aortic valve replacement with an even further improvement in her dyspnea.
References
Atkinson BJ, Cauley DH, Ng C, et al. Mammalian target of rapamycin (mTOR) inhibitor-associated non-infectious pneumonitis in patients with renal cell cancer: predictors, management, and outcomes. BJU Int 2014;113:376-82.
Baas MC, Struijk GH, Moes DJ, et al. Interstitial pneumonitis caused by everolimus: a case-cohort study in renal transplant recipients. Transpl Int 2014;27:428-36.
Motzer RJ, Escudier B, Oudard S, et al. Phase 3 trial of everolimus for metastatic renal cell carcinoma : final results and analysis of prognostic factors. Cancer 2010;116:4256-65.
Albiges L, Chamming's F, Duclos B, et al. Incidence and management of mTOR inhibitor-associated pneumonitis in patients with metastatic renal cell carcinoma. Ann Oncol 2012;23:1943-53.
Siddiqui AS, Zimmerman JL. Everolimus associated interstitial pneumonitis in a liver transplant patient. Respir Med Case Rep 2016:19:15-7.
White DA, Camus P, Endo M, et al. Noninfectious pneumonitis after everolimus therapy for advanced renal cell carcinoma. Am J Respir Crit Care Med 2010;182:396-403.
Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017;70:252-89.