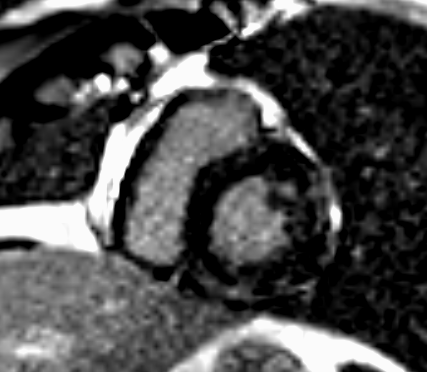
A 44-year-old active duty special operations male soldier presents with recurrent substernal chest pressure and exercise intolerance preceded by a two-week febrile, non-bloody diarrheal illness while deployed to Guatemala. Physical examination is grossly normal. Electrocardiogram demonstrates a normal sinus rhythm, diffuse ST depressions with deep T wave inversions and ST elevation in lead aVR. Laboratory evaluation reveals a troponin I of 17.3 ng/mL, an elevated c-reactive protein (CRP), and an elevated erythrocyte sedimentation rate (ESR). The patient is admitted and treated for presumed non-ST elevation myocardial infarction and receives standard medical pharmacotherapies. Invasive coronary angiography reveals no significant coronary artery disease. Echocardiogram shows a preserved ejection fraction without any wall motion abnormalities or valvular lesions. Cardiac magnetic resonance (CMR) imaging performed is shown in Figure 1.
Figure 1
Figure 1
Which of the following is most appropriate regarding the next best step in management for this soldier?
Show Answer
The correct answer is: B. Three to six months of occupational and duty restrictions with evaluation for myocarditis etiologies.
The patient's clinical history, electrocardiogram, and CMR imaging findings demonstrating patchy midwall late gadolinium enhancement (LGE) pattern are consistent with a diagnosis of myocarditis. Myocarditis in the active duty population is commonly secondary to viral illnesses, similar to the general population. Military personnel with their unique exposures are at increased risk for myocarditis secondary to chemical or pharmacological toxins, hypersensitivity reactions, small pox vaccine, and extreme temperature exposures. In this case scenario, an infectious disease evaluation for Chagas disease, HIV, and diarrheal illnesses is recommended. Myocarditis has accounted for 3.3% of sudden cardiac deaths in the military population with a propensity to affect individuals younger than 35 years of age.
Holter monitoring and graded exercise testing are routinely employed to ensure there is no evidence of arrhythmia. Military duty and occupational restriction is recommended for three to six months with observed resolution of symptoms, EKG abnormalities, and serum markers of inflammation with concurrent normalization of left ventricular function and cardiac dimensions prior to returning to duty.
Continuation of DAPT for 12 months followed by indefinite aspirin therapy would be appropriate for the treatment of acute coronary syndrome. The patient's clinical presentation, coronary angiography, and CMR are not consistent with this diagnosis.
Initiation of guideline directed medical therapy with ACE inhibitor and beta blocker would be the appropriate strategy utilized if this patient were presenting with a new heart failure syndrome. There is no clear evidence of a clinical heart failure decompensation in this presentation.
Acetylcholine provocative testing and treatment with calcium channel blockers or nitrates would be reasonable for suspicion of coronary vasospasms as the etiology. The clinical timeline and CMR findings make this diagnosis less likely.
References
Sagar S, Liu PP, Cooper LT Jr. Myocarditis. Lancet 2012;379:738-47.
Cox AT, White S, Ayalew Y, Boos C, Haworth K, McKenna WJ. Myocarditis and the military patient. J R Army Med Corps 2015;161:275-82.
Maron BJ, Udelson JE, Bonow RO, et al. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 3: hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and other cardiomyopathies, and myocarditis: a scientific statement from the American Heart Association and the American College of Cardiology. J Am Coll Cardiol 2015;66:2362-71.
Eckart RE, Shry EA, Burke AP, et al. Sudden death in young adults: an autopsy-based series of a population undergoing active surveillance. J Am Coll Cardiol 2011;58:1254-61.