A 39-year-old man presented to emergency department with sudden onset of sharp pleuritic chest pain and increasing dyspnea for three days. He denied any orthopnea, paroxysmal nocturnal dyspnea or leg swelling. He had a past medical history of hypertension, chronic kidney disease, systemic lupus erythematosus and pulmonary fibrosis. His medications included amlodipine, hydroxychloroquine, mycophenolate mofetil and prednisolone.
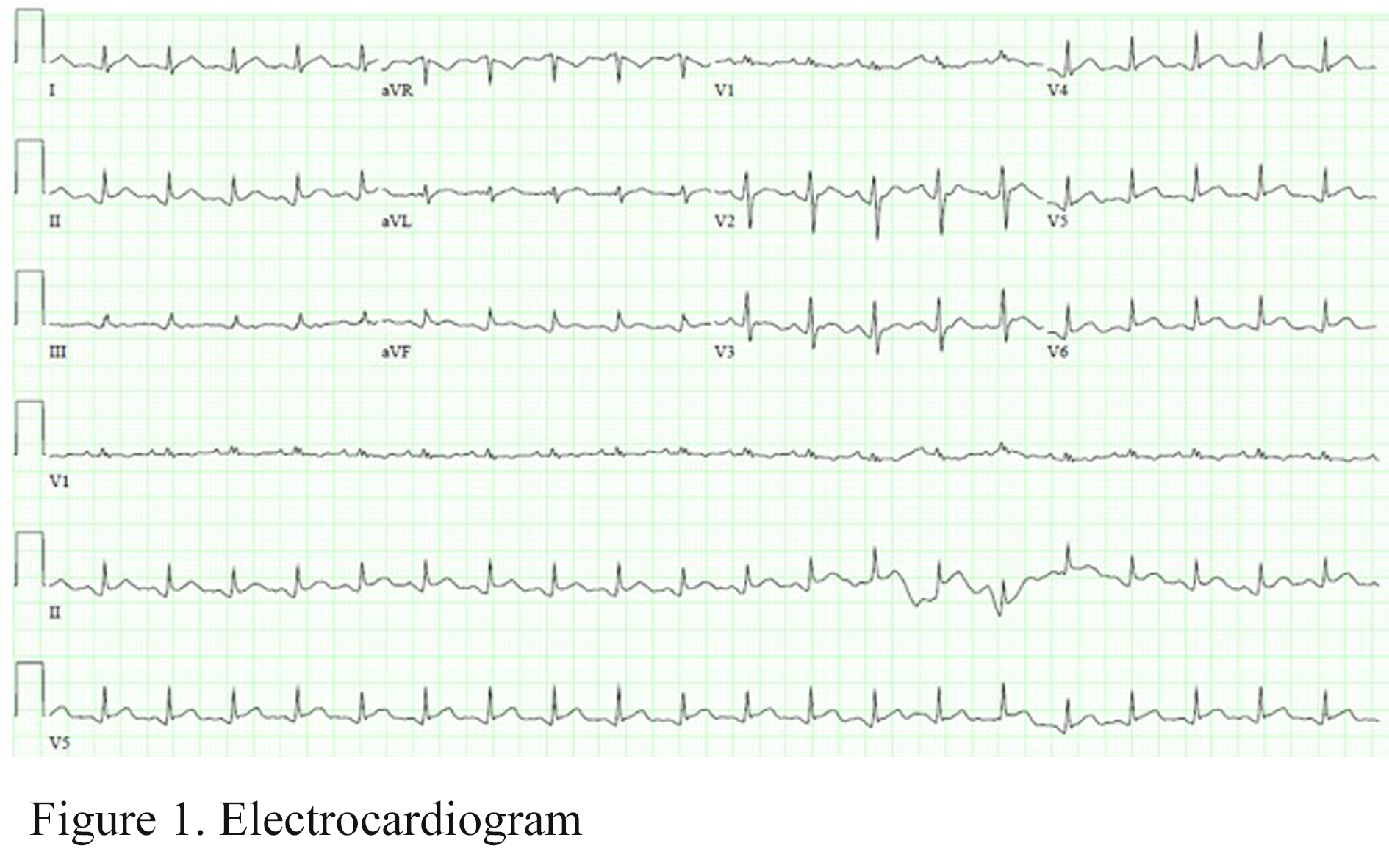
Upon admission, vital signs were notable for sinus rhythm with heart rate of 90 beats per minute, a blood pressure of 139/88 mm Hg, tachypnea with respiratory rate of 40 breaths per minute and oxygen saturation of 100% on 50% oxygen via face mask. Pericardial rub and distended jugular vein were noted on physical examination. His electrocardiogram showed ST depressions in the inferolateral leads and PR depressions in lead II and PR elevation in lead aVR (Figure 1). Cardiomegaly was shown on chest X-ray.
Figure 1
Figure 1
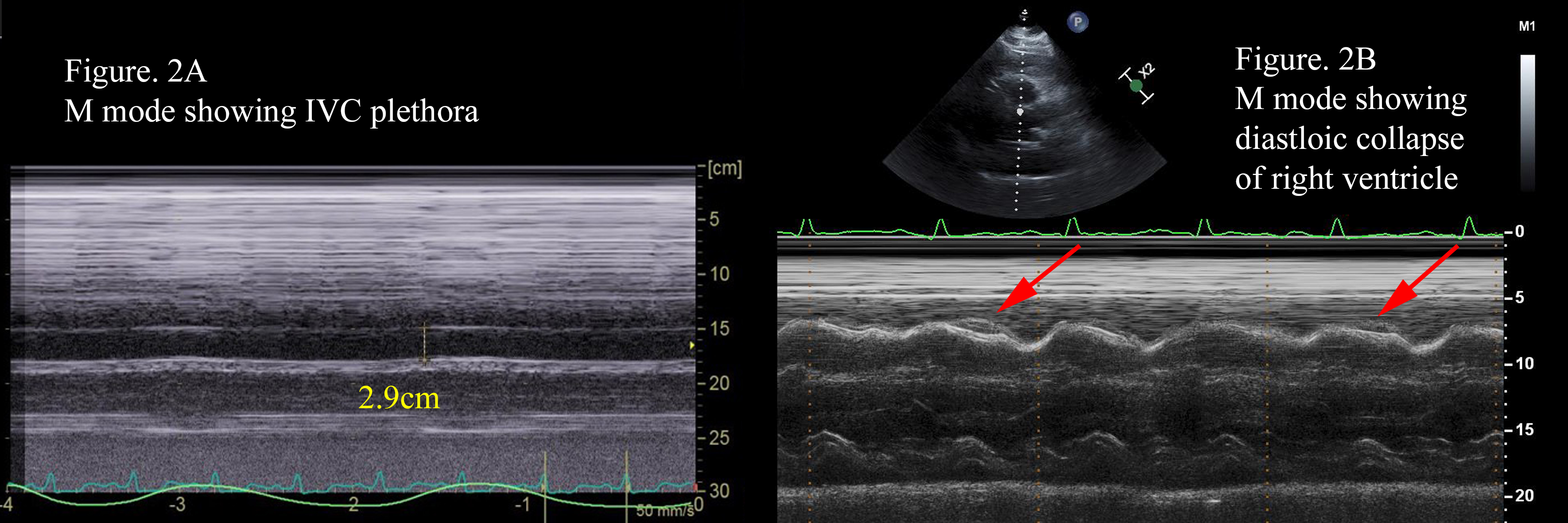
Urgent echocardiogram showed a large circumferential pericardial effusion and echocardiographic evidence of cardiac tamponade. There was significant respiratory variation in the mitral and tricuspid inflows, i.e. ~26% and ~-62% respectively. Inferior vena cava (IVC) was plethoric with a diameter of 2.9cm and no change in size during respiration (Figure 2A). There appeared diastolic collapse of right ventricular outflow tract (Figure 2B). Pericardiocentesis was then performed and yielded 600 ml slightly turbid yellowish fluid which was confirmed to be exudative.
Figure 2
Figure 2
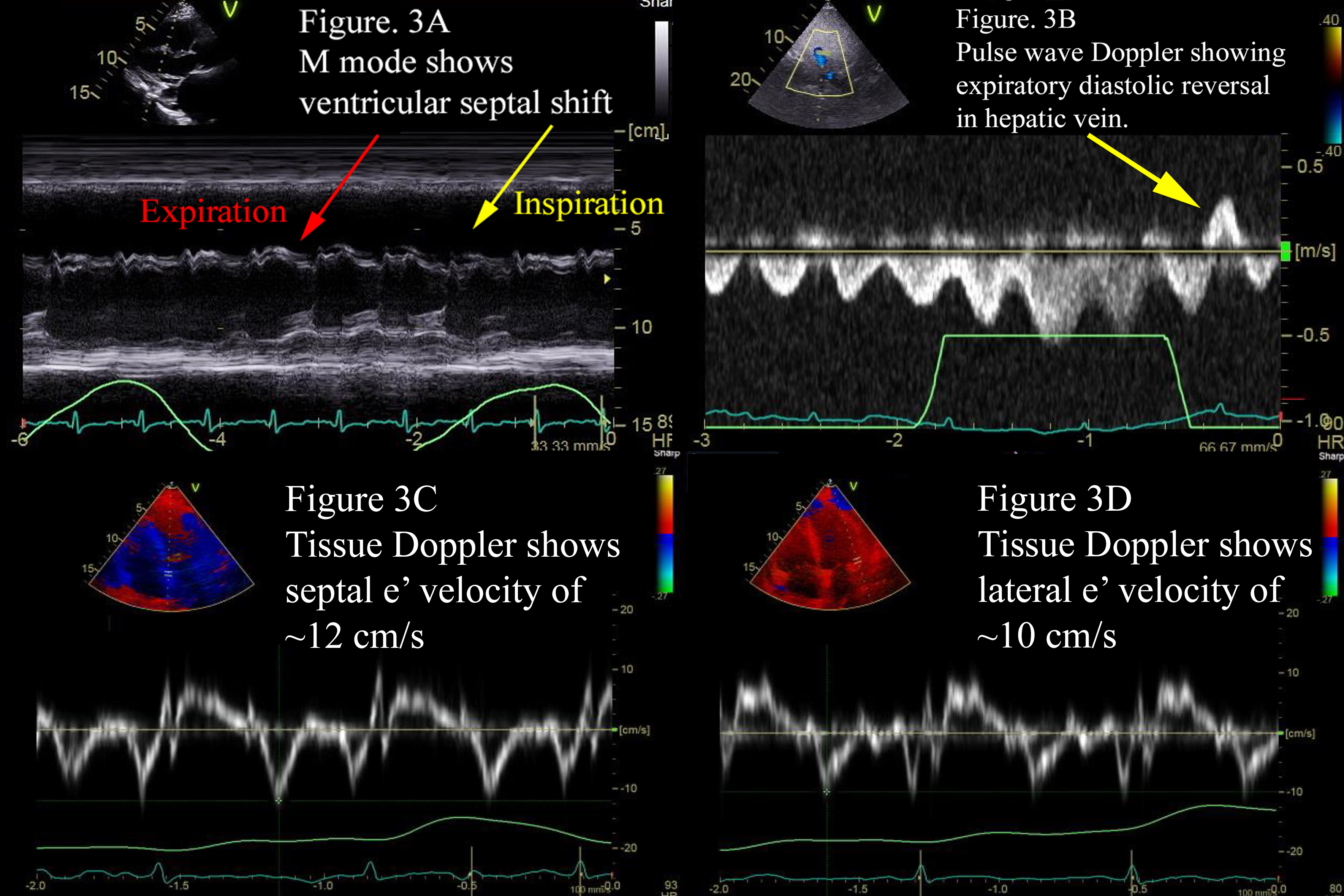
However, patient still had pleuritic chest pain after pericardiocentesis. Echocardiogram was then repeated and showed a small circumferential pericardial effusion. There was significant respiratory variation in the mitral inflow (~26%), and IVC was still plethoric, but there was no diastolic chamber collapse. There was a ventricular septal shift (i.e., cyclic movement of the ventricular septum toward the left ventricle with inspiration and towards the right ventricle with expiration) (Figure 3A). There was hepatic vein expiratory diastolic reversal (Figure 3B). Tissue Doppler imaging of mitral annulus velocities showed "annulus reversus", which the septal e' velocity (12 cm/s) was greater than the lateral one (10 cm/s) (Figure 3C, 3D).
Figure 3
Figure 3
Which of the following is the likely diagnosis?
Show Answer
The correct answer is: B. Effusive-constrictive pericarditis.
The diagnosis of effusive-constrictive pericarditis (ECP) was made based on the echocardiographic findings and was confirmed by the persistently elevated right atrial pressure by central venous pressure measurement. The dose of prednisolone was increased from 10mg daily to 60mg daily. Colchicine and ibuprofen were added. The symptoms of pleuritic chest pain improved. Repeated echocardiogram one year later showed the resolution of pericardial effusion and no evidence of constriction.
ECP was first described in the 1960s as a variant of pericarditis. Hancock defined it as a distinct pathophysiologic form of compressive pericardial disease characterized by effusion into a free pericardial space associated with constriction of the heart by the visceral pericardium.1
The hallmark of ECP is the persistence of elevated right atrial pressure after intra-pericardial pressure has been reduced to normal levels by removal of pericardial fluid. The diagnostic criterion by cardiac catheterization is that tamponade has evolved into constriction (i.e., failure of the right atrial pressure to fall by ≥ 50% or below 10 mmHg after intra-pericardial pressure is lowered to near 0 mmHg by the removal of pericardial fluid).2 For constrictive pericarditis, Welch et al. suggest respiration-related ventricular septal shift, preserved or increased septal mitral annular e' velocity, and prominent hepatic vein expiratory diastolic flow reversal as the echocardiographic diagnostic criteria of constrictive pericarditis.3 However, there is still no agreed echocardiographic criteria of diagnosing ECP at this time.4-5
Incidence of ECP ranges from 2-15% of patients with pericarditis, depending on the difference in patient populations, methodologies and definition. Cardiac surgery, idiopathic pericarditis and cardiac procedure-related pericardial effusion (e.g., pacemaker implantation and radio-frequency ablation), are the most common causes of pericardial effusion leading to ECP, which accounts for >60% of cases.2,4
Management of ECP usually starts with medical therapy including the combination of NSAID, colchicine ± corticosteroid. If medical therapy fails, pericardiectomy remains an option. Long-term prognosis in patients with ECP remains good. Pericardiectomy is rarely required (<10% of patients diagnosed ECP).2,4
Transient constrictive pericarditis is an increasingly recognized sub-type of constrictive pericarditis. The underlying pathophysiology typically relates to impaired pericardial distensibility, associated with acute or sub-acute inflammation, rather than the fibrosis or calcification often seen in chronic constrictive pericarditis. It may resolve spontaneously or with the assistance of anti-inflammatory therapy.7
Occult constrictive pericarditis is identified by normal baseline hemodynamics and normal left ventricular systolic function with a characteristic response to rapid volume infusion. Diagnosis depends specifically upon the development of typical pressure pulse morphology of constriction, loss or reversal of respiratory variation of right atrial pressure, and precise diastolic equilibration of intra-cardiac pressures.6
Sagrista-Sauleda J, Angel J, Sanchez A, Permanyer-Miralda G, Soler-Soler J. Effusive-constrictive pericarditis. N Engl J Med 2004;350:469-75.
Welch TD, Ling LH, Espinosa RE, et al. Echocardiographic diagnosis of constrictive pericarditis: Mayo Clinic criteria. Circ Cardiovasc Imaging 2014;7:526-34.
Kim KH, Miranda WR, Sinak LJ, et al. Effusive-constrictive pericarditis after pericardiocentesis: incidence, associated findings, and natural history. JACC Cardiovasc Imaging 2018;11:534-41.
van der Bijl P, Herbst P, Doubell AF. Redefining effusive-constrictive pericarditis with echocardiography. J Cardiovasc Ultrasound 2016;24:317-23.
Bush CA, STang JM, Wooley CF, Kilman JW. Occult constrictive pericardial disease. Diagnosis by rapid volume expansion and correction by pericardiectomy. Circulation 1977;56:924-30.
Gentry J, Klein AL, Jellis CL. Transient constrictive pericarditis: current diagnostic and therapeutic strategies. Curr Cardiol Rep 2016;18:41.