A 53-year-old previously active male patient with a history of cluster headaches on verapamil and no prior personal or family cardiac history presented to the emergency department with a chief complaint of 3 months of progressive dyspnea. Over the last 3 months, the patient endorsed a 15-pound weight gain, lower extremity edema, early satiety, and abdominal bloating and was now dyspneic at rest.
On physical exam, the patient had markedly elevated jugular venous pressures to 20 cm above the right atrium and clear lungs. His heart rate was regular at 94 bpm with an accentuated second heart sound and right ventricular (RV) heave. A 3/6 systolic murmur was present at the left lower sternal border, and 1+ lower extremity edema was present. His blood pressure was 117/73 mmHg, and oxygen saturation was 92% on 3 liters oxygen. Initial laboratory tests showed the following:
Aspartate aminotransferase = 704 IU/L
Alanine aminotransferase = 909 IU/L
Blood urea nirogen = 44 mg/dL
Creatinine = 2.84 mg/dL
Lactic acid = 9.8 mmol/L
Troponin = 0.02 ng/mL
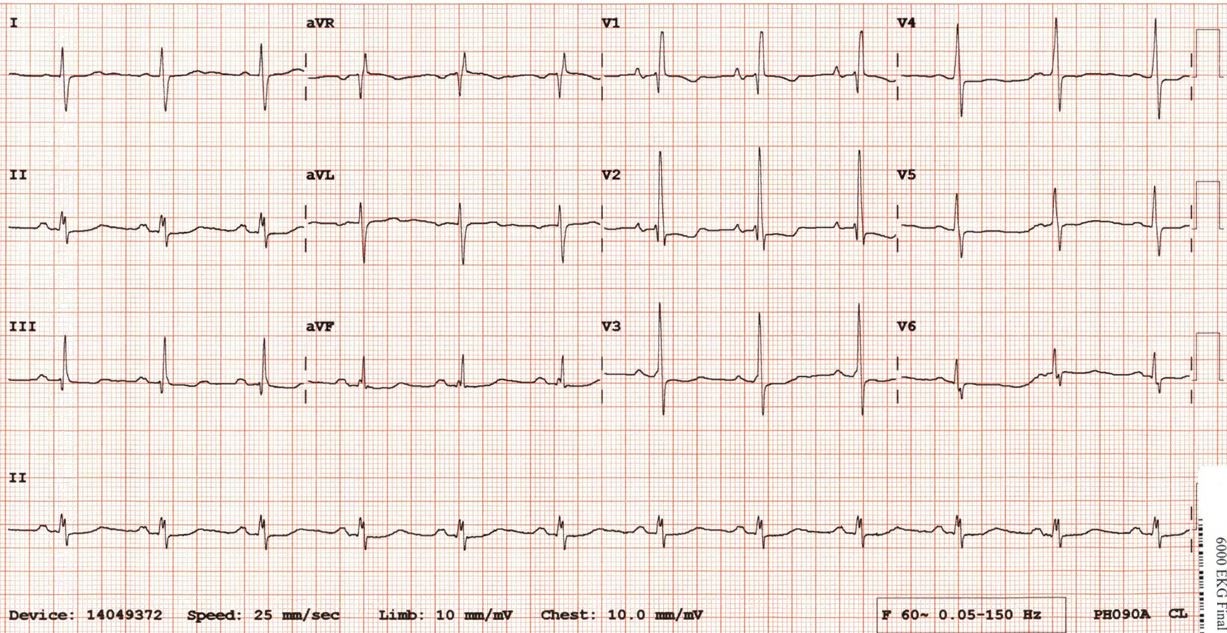
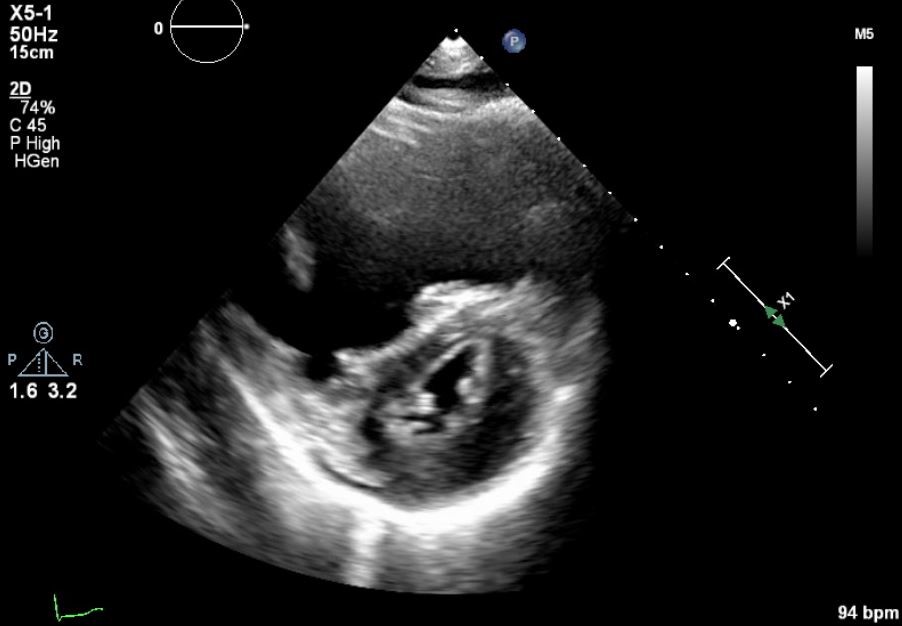
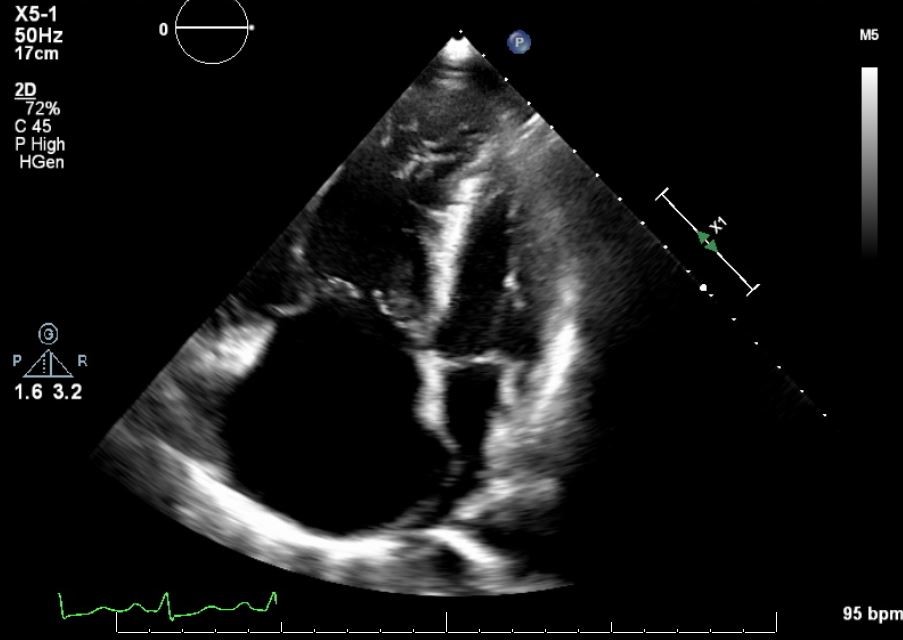
An electrocardiogram (ECG) and echocardiogram are shown in Figures 1-3. The ECG was notable for severe RV hypertrophy with RV strain and echocardiogram demonstrated severe RV enlargement and dysfunction. The patient underwent a ventilation perfusion scan, which showed low probability for pulmonary embolism.
Figure 1
Figure 1
Figure 2
Figure 2
Figure 3
Figure 3
What is the best next step in management of this patient's symptoms?
Show Answer
The correct answer is: D. Right heart catheterization (RHC) to assess hemodynamics
PAH encompasses a group of pulmonary vascular disorders characterized hemodynamically by mean pulmonary artery (PA) pressure >20 mmHg, pulmonary capillary wedge pressure ≤15 mmHg, and pulmonary vascular resistance ≥3 Wood units in the absence of other causes of elevated PA pressures.1-4 Diagnosis of PAH requires a high index of suspicion, especially in patients with no apparent risk factors, like the patient in this case. The patient has features of severe RV failure with congestive hepatopathy and acute kidney injury secondary to cardiorenal syndrome. Diagnosis of PAH is based on hemodynamic measurements with RHC. Assessment of the vasodilator response with inhaled nitric oxide is recommended to identify the <7% of patients who benefit from treatment with calcium channel blockers (CCBs).3 A coronary angiogram is not indicated at this time. The patient's history and ECG make ischemic etiology less likely, and he would be at increased risk of contrast-induced kidney injury and myocardial depression given his decompensated state and markedly elevated right atrial pressures.
The patient does not have systemic hypotension, and optimization with diuretics and RV afterload reduction should be pursued before inotropes.
RV support with percutaneous ventricular assist device is not recommended because less-invasive measures have not yet been attempted, and mechanical support does not treat the primary pulmonary vascular disease.
Nicardipine is a dihydropyridine CCB and does not have the same negative inotropic effects as the non-dihydropyridine CCB verapamil, but the patient has not yet had a vasodilator challenge and so should not empirically be started on a CCB.
Patients with PAH have poor survival,5 and survival remains poor despite treatment advances over the last decade.6 Age, PAH etiology, World Health Organization functional class, pericardial effusion, 6-minute walk test distance, and brain natriuretic peptide are predictors of prognosis in PAH and help identify a phenotype of patients who benefit from aggressive upfront therapy.6,7 In addition to his evidence of hypoperfusion and multisystem organ dysfunction from his RV failure on presentation, the patient had elevated brain natriuretic peptide (537 pg/ml) even after 10 days of PAH therapy. His 6-minute walk test distance was <150 meters, clearly classifying him as benefitting from upfront combination therapy, which has been shown to significantly improve hemodynamics, RV function, and morphology compared with monotherapy.8
The patient underwent RHC with vasodilator challenge. RHC revealed right atrial pressure of 20 mmHg, PA pressues of 90/40 mmHg with mean PA pressures of 57 mmHg, and pulmonary capillary wedge pressure of 15 mmHg. Fick cardiac output was 4.1 L/min with cardiac index of 2.48 L/min/m2 based on a PA saturation of 68% and aortic saturation 93%. With 100% oxygen and inhaled nitric oxide challenge, the patient had no significant vasodilator response. The patient was diuresed and started on initial combination therapy with riociguat and intravenous treprostinil. His renal function and hepatic function normalized. With medical optimization, the patient was able to be weaned off of supplemental oxygen and was discharged home with plan to start an endothelin receptor antagonist after treprostinil optimization and sustained resolution of his transaminitis.
References
Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J 2019;53:1801913.
Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016;37:67-119.
McLaughlin VV, Shah SJ, Souza R, Humbert M. Management of pulmonary arterial hypertension. J Am Coll Cardiol 2015;65:1976-97.
Konstam MA, Kiernan MS, Bernstein D, et al. Evaluation and Management of Right-Sided Heart Failure: A Scientific Statement From the American Heart Association. Circulation 2018;137:e578-e622.
Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 2010;122:164-72.
Farber HW, Miller DP, Poms AD, et al. Five-Year outcomes of patients enrolled in the REVEAL Registry. Chest 2015;148:1043-54.
Batal O, Khatib OF, Dweik RA, Hammel JP, McCarthy K, Minai OA. Comparison of baseline predictors of prognosis in pulmonary arterial hypertension in patients surviving ≤2 years and those surviving ≥5 years after baseline right-sided cardiac catheterization. Am J Cardiol 2012;109:1514-20.
Badagliacca R, Raina A, Ghio S, et al. Influence of various therapeutic strategies on right ventricular morphology, function and hemodynamics in pulmonary arterial hypertension. J Heart Lung Transplant 2018;37:365-75.