A 46-year-old woman is admitted with cardiogenic shock. She has a history of nonischemic cardiomyopathy secondary to remote chemotherapy and radiation-related cardiotoxicity following treatment of Hodgkin's lymphoma 25 years earlier. Due to radiation-induced valve injury, she underwent mitral and tricuspid valve repair a decade ago. She was hospitalized several times in recent months for decompensated heart failure (HF) despite escalation of oral diuretic dosing, suffering a progressive decline in her functional status (New York Heart Association Class IV). Attempts at uptitration and optimization of outpatient HF guideline-directed medical therapy was limited by symptomatic hypotension and neurohormonal blockade intolerance.
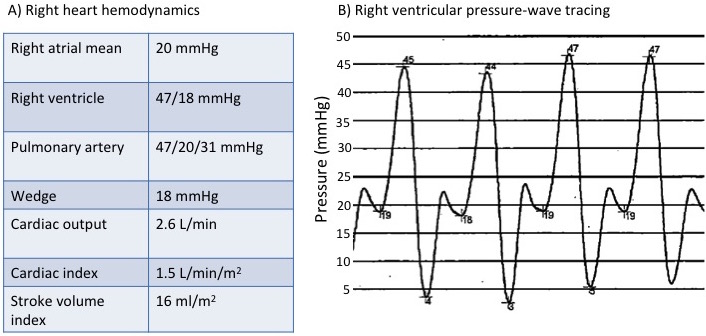
Right heart catheterization performed on presentation demonstrated reduced cardiac index, severely elevated filling pressures with increased pulmonary artery pressures, and evidence of a "square root sign" on the right ventricular pressure tracing (Figure 1). Transthoracic echocardiogram was significant for the following:
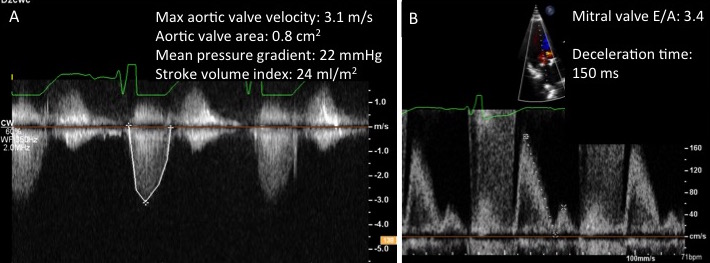
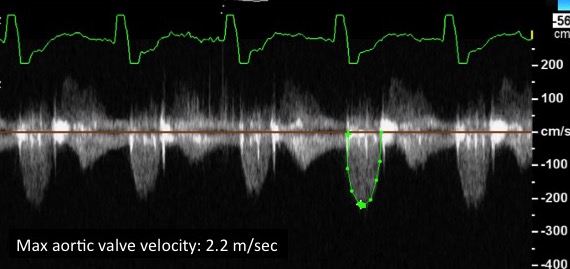
Calcified aortic valve with limited leaflet mobility (Videos 1-2) and increased peak aortic valve velocities (Figure 2A)
Restrictive left ventricular filling pattern (Figure 2B)
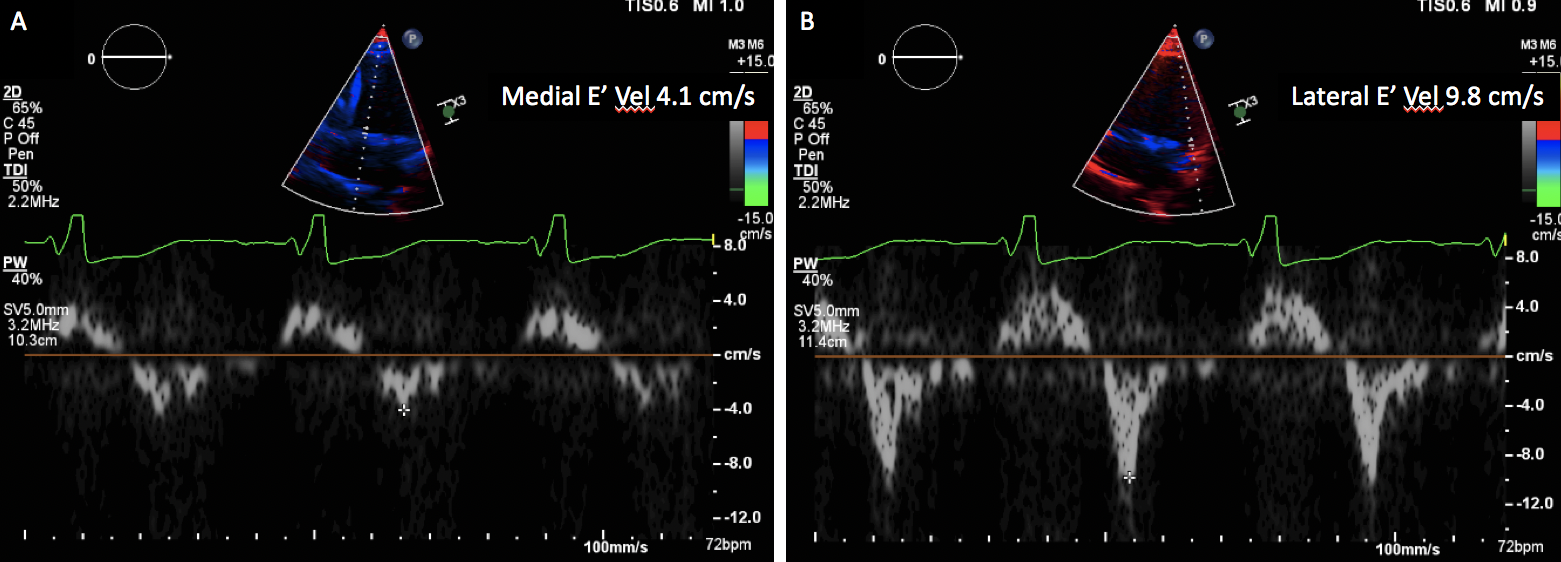
Reduced septal and lateral mitral annular tissue Doppler velocities (Figure 3) with significantly increased E/e' ratio of 26
Moderate right ventricular dysfunction
A nondilated left ventricle
Left ventricular ejection fraction of 49%
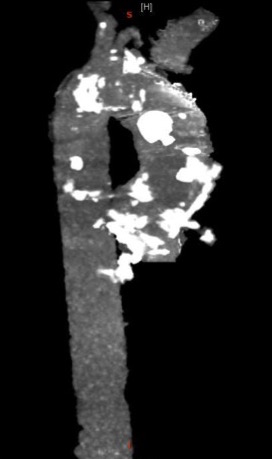
A computed tomography (CT) angiogram was notable for substantial aortic root and ascending aorta calcification (Figure 4) without significant pericardial calcification. The patient was stabilized in the cardiac intensive care unit with continuous inotropic infusion and intravenous diuretics. She had good augmentation in urine output but remained volume overloaded with ongoing low cardiac output despite attempts at optimization and inotropic support.
What is the next best step in the evaluation of this patient?
Show Answer
The correct answer is: B. Initiate discussion and evaluation for possible heart transplantation
This patient has end-stage restrictive cardiomyopathy with progressive outpatient decline in functional status and frequent readmissions for decompensated HF and now has documented low cardiac output. Initiating an evaluation for advanced HF therapies, such as heart transplantation, is the most appropriate next step at this time due to the multifactorial nature of her cardiac disease with valvular involvement, right ventricular dysfunction, and restrictive cardiomyopathy.
Surgical aortic valve replacement would be high risk due to her calcium deposition and prior sternotomy and would not address the restrictive nature of her HF. There is no convincing evidence for pericardial constriction, so stripping is not recommended (answer A is incorrect). Arranging outpatient home inotrope infusion as destination therapy before considering advanced HF therapies or engaging in a thorough discussion of the patient's goals of care is not optimal given her young age (answer C is incorrect). Due to her non-dilated left ventricle, a left ventricular assist device is not a good bridge option for her.1 If she does require mechanical circulatory support as bridge-to-transplant, a total artificial heart could be considered, but the additional sternotomy would increase her risk further (answer D is incorrect).
Cardiovascular effects from radiation can present years to decades after treatment and result in a wide spectrum of cardiovascular complications, including myocardial fibrosis, coronary artery disease, valvular heart disease, aortic calcification, carotid stenosis, pericardial disease, and conduction system dysfunction.2,3 Diffuse myocardial fibrosis from radiation therapy can result in varying degrees of diastolic dysfunction, and more advanced stages of fibrosis can lead to a restrictive cardiomyopathy.4 Concurrent exposure to chemotherapeutic agents, particularly anthracyclines, increases the likelihood of developing systolic dysfunction.5 Valvular heart disease is frequently seen in patients with radiation-associated heart disease. Aortic valve involvement is more common compared with mitral and tricuspid valves, and there is an increased frequency of aortic valve disease with time from initial irradiation.6
There are several findings of radiation-associated cardiac disease in this case, resulting in aortic stenosis and restrictive cardiomyopathy. The increased E to A ratio of mitral inflow velocities with short deceleration time (Figure 2B), significantly elevated filling pressures (Figure 1A), and "square root sign" on the right ventricular pressure tracing (Figure 1B) are consistent with restrictive left ventricular filling. Prominent aortic and valvular calcification with aortic stenosis is also seen on CT (Figure 4) and echocardiographic imaging (Videos 1-2), respectively. In the setting of this patient's restrictive cardiomyopathy and reduced stroke volume index (<35 ml/m2), the Doppler-derived hemodynamic assessment of the aortic valve (Figure 2A) is consistent with low-flow, low-gradient moderate to severe aortic stenosis. In light of this finding, the patient was evaluated for aortic valve replacement as a temporizing measure and a bridge to advanced HF work-up. Due to high surgical risk related to acute decompensation, aortic calcification, and prior sternotomy, the patient underwent a successful transcatheter aortic valve replacement (TAVR). The transcatheter aortic valve was well-seated post-deployment (Video 3) and demonstrated a normal hemodynamic profile (Figure 5). After TAVR, she stabilized clinically and was discharged home on inotropic therapy with milrinone. She is undergoing evaluation for heart transplantation.
Video 3: Intraoperative Transesophageal Echocardiogram Post-TAVR
Figure 4: CT of the Thoracic Aorta
Figure 4
Figure 5: Spectral Doppler of TAVR
Figure 5
References
Grupper A, Park SJ, Pereira NL, et al. Role of ventricular assist therapy for patients with heart failure and restrictive physiology: Improving outcomes for a lethal disease. J Heart Lung Transplant 2015;34:1042-9.
Nielsen KM, Offersen BV, Nielsen HM, Vaage-Nilsen M, Yusuf SW. Short and long term radiation induced cardiovascular disease in patients with cancer. Clin Cardiol 2017;40:255-61.
Long-Term Follow-up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers (Children's Oncology Group website). Version 4.0. October 2013. Available at http://www.survivorshipguidelines.org/pdf/LTFUGuidelines_40.pdf. Accessed 12/31/2017.
Armstrong GT, Joshi VM, Ness KK, et al. Comprehensive Echocardiographic Detection of Treatment-Related Cardiac Dysfunction in Adult Survivors of Childhood Cancer: Results From the St. Jude Lifetime Cohort Study. J Am Coll Cardiol 2015;65:2511-22.
Heidenreich PA, Hancock SL, Lee BK, Mariscal CS, Schnittger I. Asymptomatic cardiac disease following mediastinal irradiation. J Am Coll Cardiol 2003;42:743-9.