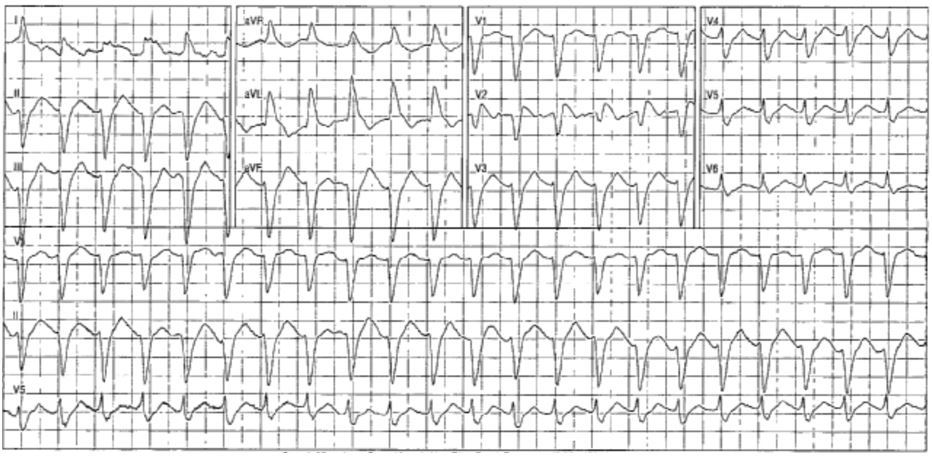
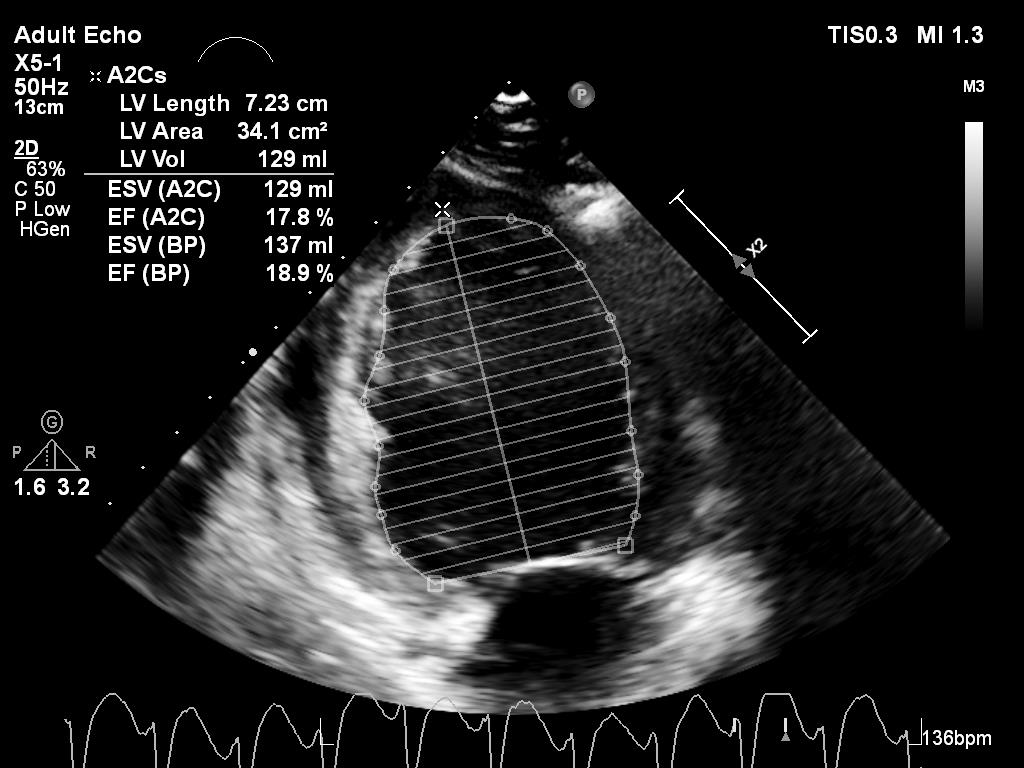
A 24-year-old female patient with recently diagnosed colorectal cancer underwent folinic acid, fluorouracil (5-FU), and oxaliplatin infusion and 24-36 hours later presented with nausea and vomiting. She was found to be tachycardic with a heart rate in the 120-130 range and blood pressure of 100/70. She was initially admitted to the oncology service with concerns for dehydration and plans for intravenous fluid resuscitation. She acutely decompensated shortly thereafter with hypotension requiring vasopressors, a wide complex tachycardia (Figure 1), acute kidney injury requiring continuous renal replacement therapy, and encephalopathy requiring intubation. A STAT echocardiogram revealed biventricular failure with left ventricular ejection fraction of 15% (Figure 2).
Figure 1
Figure 1
Figure 2
Figure 2
What is the best course of treatment for this patient?
Show Answer
The correct answer is: D. Uridine triacetate
It has been demonstrated clinically and in animals that uridine prevents or reduces 5-FU-related mortality and toxicity to the gastrointestinal tract and hematopoietic system. When it is administered after 5-FU infusion, uridine competes with the toxic 5-FU metabolite fluorouridine triphosphate for incorporation into RNA in normal tissues. Clinical studies have shown that the administration of uridine significantly improved survival in models of 5-FU overdosing or clearance defects, especially when it was administered within the first 24 hours after 5-FU infusion (Figure 3).1,4-5
Figure 3
Figure 3
Studies have shown a reported incidence of symptomatic cardiotoxicity (defined as chest pain, arrhythmia, electrocardiographic changes, myocardial infarction, myocarditis, or heart failure) anywhere between 0% and 20%. However, cardiogenic shock, heart failure, and myocardial infarction are much less common, with a reported incidence of 0-2%. Cardiotoxicity may occur within 12 hours following treatment initiation, although animal studies have shown it occurring as late as 48 hours post-treatment.1-3
There have not been many studies regarding the use of uridine triacetate and severe cardiotoxicity, such as in this case; therefore, there is no clear recovery timeline in this patient population. Further studies need to be performed.
References
Ma WW, Saif MW, El-Rayes BF, et al. Emergency use of uridine triacetate for the prevention and treatment of life-threatening 5-fluorouracil and capecitabine toxicity. Cancer 2017;123:345-56.
Polk A, Vaage-Nilsen M, Vistisen K, Nielsen DL. Cardiotoxicity in cancer patients treated with 5-fluorouracil or capecitabine: a systematic review of incidence, manifestations and predisposing factors. Cancer Treat Rev 2013;39:974-84.
Sorrentino MF, Kim J, Foderaro AE, Truesdell AG. 5-fluorouracil induced cardiotoxicity: review of the literature. Cardiol J 2012;19:453-8.
Andreica IW, Pfeifer E, Rozov M, Tavares E, Shakurova A, Ortiz T. Fluorouracil overdose: clinical manifestations and comprehensive management during and after hospitalization. J Hematol Oncol Pharm 2015;5:43-7.
Bamat M, Tremmel R, Helton J, von Borstel R. Clinical experience with uridine triacetate for 5-fluorouracil overexposure: An update. Ann Oncol 2013;24(Suppl 4):iv71.