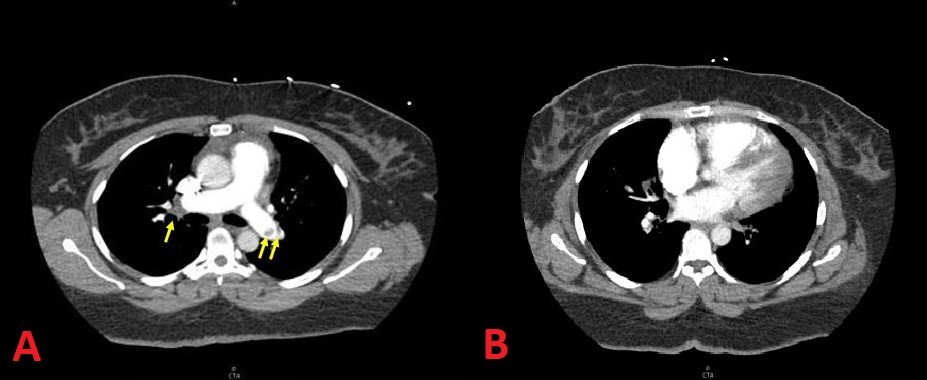
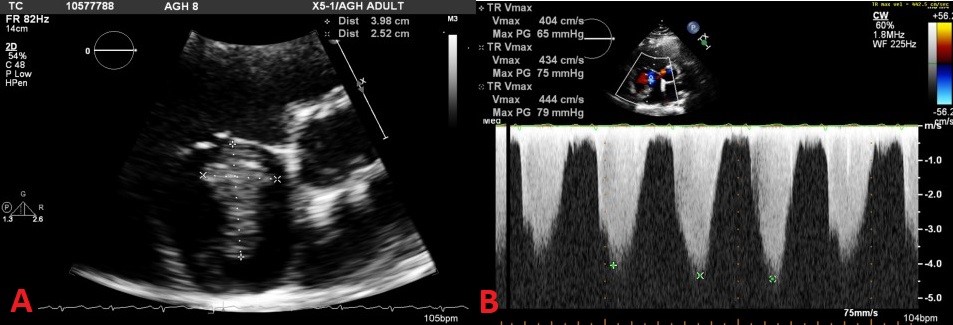
A 42-year-old female patient with a medical history significant for type 2 diabetes mellitus presented to the hospital with a 1-week history of new-onset exertional dyspnea. Her vital signs were blood pressure of 118/72 mmHg, heart rate of 92 bpm, and O2 saturation of 98% (2L nasal cannula). The patient's initial physical exam was largely unremarkable, with the exception of jugular venous distention estimated at 12 cm of water. A chest X-ray was negative for any acute process. Computed tomography angiography (CTA) demonstrated central pulmonary emboli present in both pulmonary arteries as well as in sub-segmental branches of the right upper lobe, right middle lobe, and both lower lobes (Figure 1). The right ventricle/left ventricle ratio was calculated at 1.7. Transthoracic echocardiogram revealed a large, mobile right atrial (RA) thrombus measuring 4.3 x 2.2 cm (Figure 2A). In addition, there was significant right ventricular dysfunction and severely elevated pulmonary artery (PA) pressure >90 mmHg with normal left ventricular and left atrial size and function (Figure 2B). Troponin was <0.01.
Figure 1
Figure 1
Figure 2
Figure 2
What are the correct diagnosis and the most appropriate next step in this patient's treatment?
Show Answer
The correct answer is: D. Acute on chronic PE; start anticoagulation and assess for pulmonary thromboendarterectomy after 3 months
Answers A, B, and C are incorrect. Although the patient does have an acute PE, her mean PA pressure is very high (out of proportion to transient rise in PA pressure typically seen in acute PE). In addition to an acute PE, her CTA demonstrated pulmonary web formation in the left and right lower lobe branches. Although her RA mass could represent a clot in transit, it was actually a highly organized thrombus (Figure 3, with the RA mass placed in the middle).
Figure 3
Figure 3
Intracardiac thrombus is a relative contraindication to thrombolytic therapy (answer C). Answer B (aspiration thrombectomy) is also not ideal because it carries significant risk of distal and proximal embolization. Though the need to quickly intervene on a massive RA thrombus is instinctively tempting, this patient was hemodynamically stable on presentation, requiring only minimal supplemental oxygen, without tachycardia or hypotension. As such, there is no indication for the aforementioned therapies. Further diagnostic studies, including right heart catheterization, pulmonary angiography, and ventilation perfusion (V/Q) scintigraphy should be deferred. Instrumentation is largely contraindicated in the setting of large RA clot, and V/Q would not add any diagnostic value or change management at this time.
Answer E is incorrect. Chronic thromboembolic pulmonary hypertension is defined as elevated PA pressures with persistent perfusion defects after at least 3 months of anticoagulation. This patient needs outpatient anticoagulation (for acute PE) followed by V/Q scanning and operability assessment for pulmonary thromboendarterectomy at an experienced center for her underlying chronic disease burden.
References
Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J 2015;46:903-75.
Gerges C, Skoro-Sajer N, Lang IM. Right ventricle in acute and chronic pulmonary embolism (2013 Grover Conference series). Pulm Circ 2014;4:378-86.
Konstantinides SV, Torbicki A, Agnelli G, et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J 2014;35:3033-69.