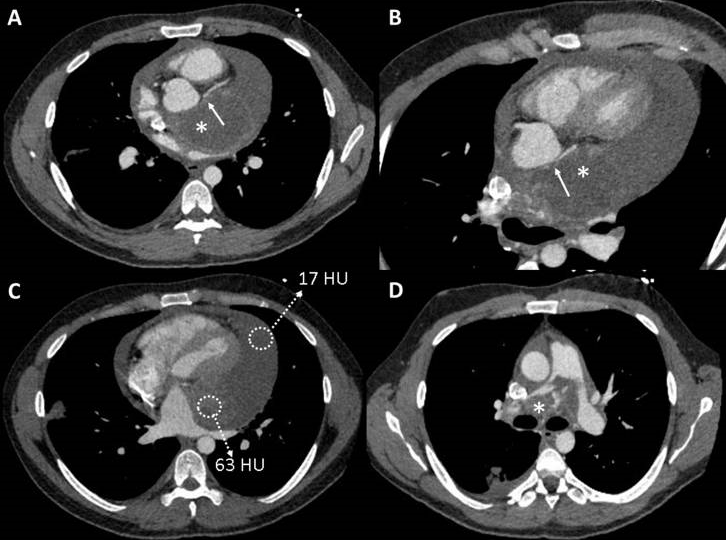
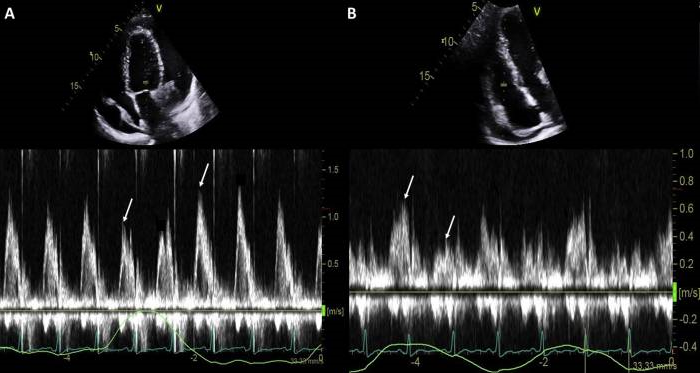
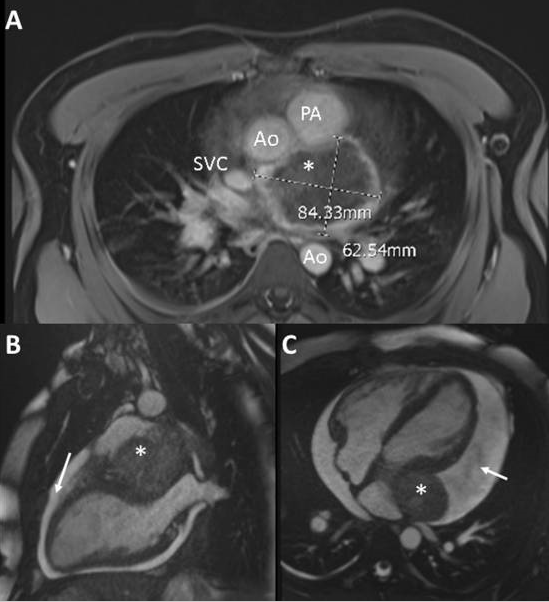
A 30-year-old man presented to the emergency department with progressive exertional dyspnea and pleuritic chest pain. His medical, surgical, social, and family histories were unremarkable for any cardiovascular disease or associated risk factors. He was treated for a pneumonia with a macrolide 3 weeks ago. Computed tomography (CT) (Figure 1) of the chest revealed a large soft tissue density mass (6.9 × 6.1 cm, 30–60 Hounsfield units), extending from the level of the left atrium and lateral mitral annulus superiorly to the posterolateral aspect of the aortic root and main PA. Transthoracic echocardiography demonstrated a large pericardial effusion with a large extrinsic left atrial mass, adjacent to the main PA and the left sinus of Valsalva. Left ventricular ejection fraction was preserved (67%), without major valvular abnormalities. The inspiratory flow variations across the mitral and tricuspid valves were 58% and 64%, respectively (Figure 2). Cardiac magnetic resonance imaging (Figure 3) demonstrated a large mass invading the main and right PAs, resulting in severe intraluminary obliteration. In addition, a large right lower lobe pulmonary infarct was also noted. The patient was admitted to the cardiac intensive care unit for closer monitoring due to signs of pre-tamponade physiology.
Figure 1
Figure 1
Figure 2
Figure 2
Figure 3
Figure 3
Which of the following is the best next step in management of this patient?
Show Answer
The correct answer is: C. Urgent radical resection of intracardiac mass and intra-operative pericardial drainage.
Primary cardiac tumors are rare and have been found in 0.0017%–0.28% of autopsies in the general population.1 About 25% of primary cardiac tumors are malignant, with cardiac sarcomas accounting for 75% of primary malignant cardiac tumors. Because of the rarity of the condition, there is a scarcity of data to guide diagnosis and management of complex masses and concern for hemodynamic compromise.1-3
The patient was admitted to the cardiac intensive care unit in preparation for surgical resection of the cardiac mass. Although the correct answer provided is C. Urgent radical resection of intracardiac mass and pericardial drainage, the patient underwent emergent pericardiocentesis given pre-tamponade physiology in an attempt to optimize hemodynamics before surgery, to avoid sudden hemodynamic collapse during induction with general anesthesia. Four hours following pericardiocentesis, the patient went into polymorphic ventricular tachycardia which degenerated into ventricular fibrillation (Figure 5). Return of spontaneous circulation (ROSC) was achieved within 3 minutes.
Figure 4
Figure 4
Figure 4: (A) Baseline electrocardiogram (B) Electrocardiogram obtained during an episode of resting chest pain, 4 hours after pericardiocentesis.
Figure 4: (A) Baseline electrocardiogram (B) Electrocardiogram obtained during an episode of resting chest pain, 4 hours after pericardiocentesis.
Repeat transthoracic echocardiography at this stage demonstrated resolution of the pericardial effusion. However, left ventricular ejection fraction appeared to be significantly depressed (30%–35%), with interval development of severe hypokinesis in the left anterior descending coronary artery (LAD) territory. Emergent left-heart catheterization revealed a separate LAD ostium from the left coronary sinus, with severe ostial narrowing and angiographic appearance concerning for extrinsic compression. An intra-aortic balloon pump was inserted, and the patient underwent urgent median sternotomy with radical resection of the mass, lymph nodes, PAs, and entire right lung.
Tumors arising from the ventricular myocardium have been reported to cause arrhythmias and sudden cardiac death due to obstructed blood flow. In our case, we believe the patient went into ventricular fibrillation arrest soon after pericardiocentesis because of extrinsic compression of the LAD by the large PAS mass, following disruption of the cushioning effect provided by the large pericardial effusion. In retrospect, expedited surgery and intra-operative pericardial drainage may have mitigated the risk of such an event.
The location of the sarcoma not only determines the clinical presentation but also survival, morbidity, surgical approach, and perioperative mortality.2 Pulmonary artery sarcomas present with vague clinical signs and symptoms such as chest pain, dyspnea, hemoptysis, cough, constitutional symptoms, and/or right-sided heart failure. Diagnosis can hence be delayed for as long as 3-12 months.3 Surgical resection involving replacement of the PA and possible pneumonectomy to obtain adequate margins remains the mainstay treatment to prolong survival, though there are no specific guidelines for its management.3-4 PAS is poorly responsive to chemotherapy and radiation.3 Multimodality treatment has been shown to improve outcomes, with median survival of 24.7 ± 8.5 months compared with 8.0 ± 1.7 months for single-modality therapy.3,5 Given the limited management options, aggressive nature of disease, and potential delay in diagnosis, prognosis continues to remain grim with median survival of 36.5 ± 20.2 months after curative surgery compared with 11 ± 3 months for incomplete resection.5 Most common causes of death include right-sided heart failure from right ventricular outflow obstruction, and distant metastases.6
References
Shanmugam G. Primary cardiac sarcoma. Eur J Cardiothorac Surg. 2006;29:925–32
Burke A., Jeudy J., Virmani R. Cardiac tumours: an update. Heart. 2008;94:117–23