A 26-year-old woman with a history of secundum atrial septal defect and patent ductus arteriosus (PDA) for which she underwent surgical closure 23 years prior to presentation followed by coil closure of a recanalized PDA 10 years later with a stainless steel coil was seen in clinic for recurrent pleuritic chest pain.
She describes five prior episodes of pleuritic chest pain radiating to her right shoulder over the past 4 years. During her fourth episode she was evaluated by a local cardiologist and was found on exam to have a pericardial friction rub, PR depressions on electrocardiogram (ECG) and a small pericardial effusion on echocardiogram. With all four diagnostic criteria met, she was diagnosed with acute pericarditis and started on colchicine and ibuprofen. She reports taking ibuprofen for approximately one week until her symptoms resolved and was gradually tapered off colchicine over three months. Her fifth and most recent episode of pleuritic chest pain occurred two months prior to presentation. She was again seen by her local cardiologist and lab work was notable for elevated erythrocyte sediment rate (ESR) and C-reactive protein (CRP). She was restarted on colchicine and non-steroidal anti-inflammatory medications. Her symptoms resolved within two weeks and she self-discontinued both medications.
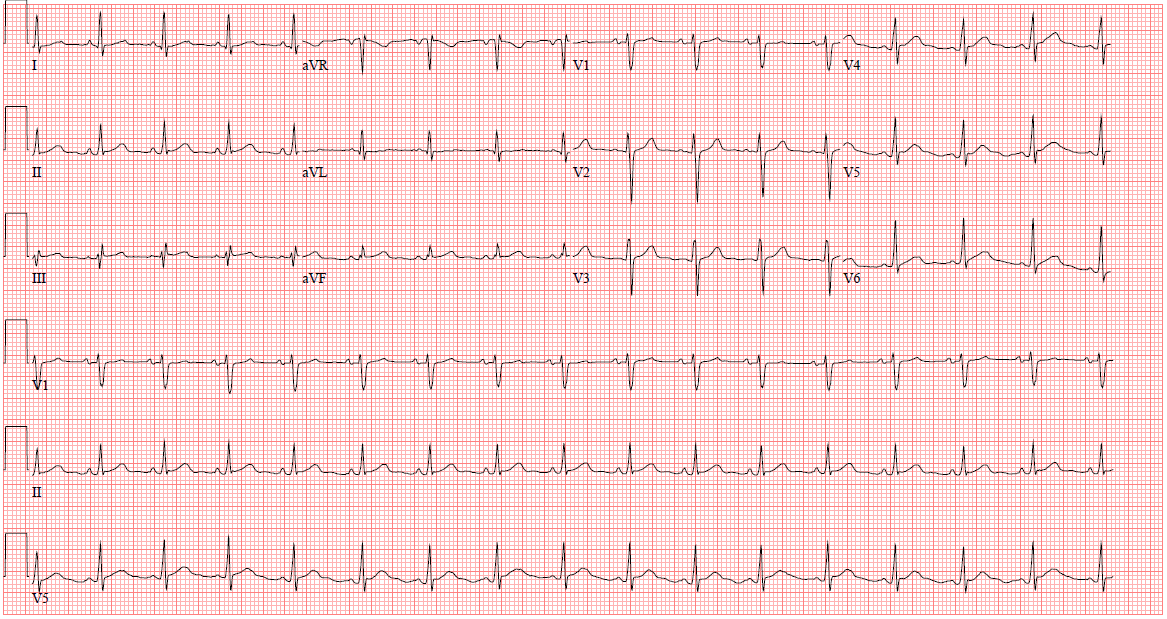
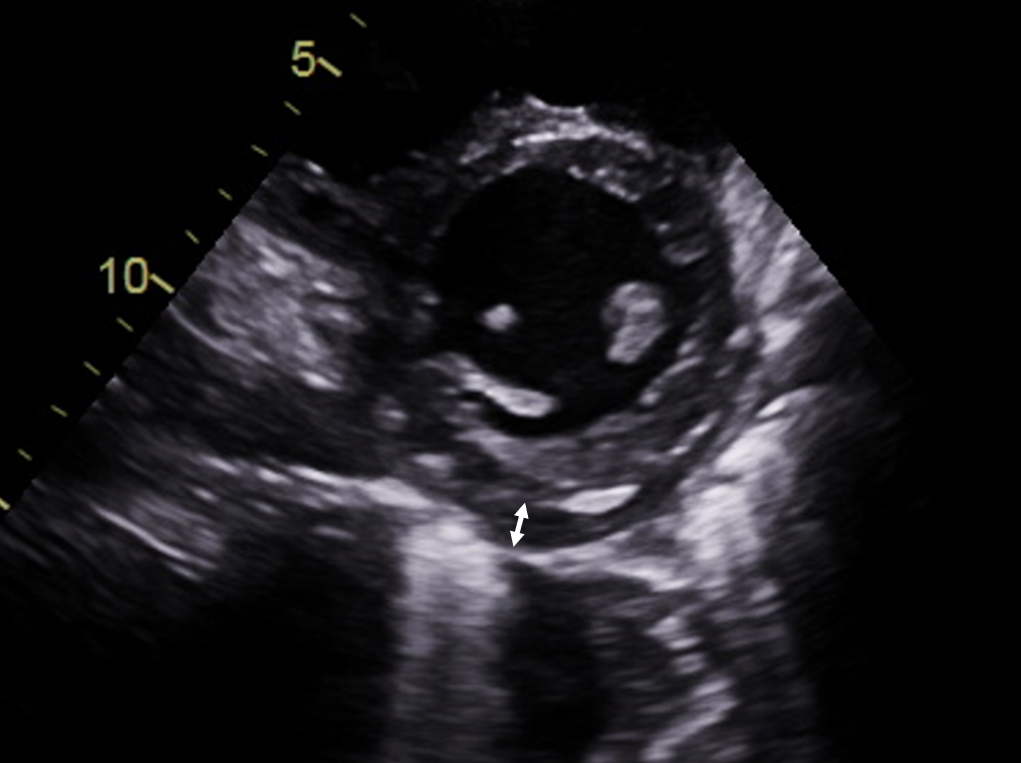
On current presentation she endorsed severe pleuritic chest pain radiating to her upper back that started several days prior. On exam she was febrile to 102.7 degrees Fahrenheit, her blood pressure was 129/60 mmHg and she was tachycardic to 116 beats per minute. Her cardiac exam was remarkable for a pericardial friction rub. Her labs were notable for a white blood cell count of 17 (normal range 3.7-11.0 k/uL), ESR of 71 mm/hr (normal <20 mm/hr) and CRP of 33.5 (normal <0.9 mg/dL). Her ECG (Figure 1) demonstrated subtle diffuse J point elevation and sub-millimeter PR depressions most pronounced in the inferior leads. Echocardiogram (Figure 2) demonstrated a small circumferential pericardial effusion (0.8 cm), a normal appearing inferior vena cava measuring 1.6 cm with greater than 50 percent collapsibility with inspiration, right atrial tethering with respirophasic shift of the intraventricular septum and a diastolic septal bounce suggestive of early effusive-constrictive physiology.
She was admitted for management of acute recurrent pericarditis. Given her history of recurrent pericarditis, additional imaging was pursued to assess the degree of pericardial inflammation. Delayed enhancement imaging after administration of intravenous gadolinium on cardiac magnetic resonance (CMR) is typically the modality of choice to characterize the pericardium. However, given the presence of her prior PDA coil, CMR could not be obtained. She subsequently underwent 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) imaging.
Figure 1
Figure 1
Figure 1: Electrocardiogram Demonstrating Subtle Diffuse J point elevation and Sub-Millimeter PR Depressions, Most Prominent in the Inferior Leads
Figure 1: Electrocardiogram Demonstrating Subtle Diffuse J point elevation and Sub-Millimeter PR Depressions, Most Prominent in the Inferior Leads
Figure 2
Figure 2
Figure 2: Parasternal Short Axis View on Transthoracic Echocardiogram Showing a Small Pericardial Effusion Measuring 0.8 cm (white arrow)
Figure 2: Parasternal Short Axis View on Transthoracic Echocardiogram Showing a Small Pericardial Effusion Measuring 0.8 cm (white arrow)
Which of the following findings on 18F-FDG PET imaging is suggestive of acute pericarditis?
Show Answer
The correct answer is: D. Diffuse pericardial FDG uptake.
PET with 18F-FDG is routinely used to assess for the presence of myocardial inflammation in cases of sarcoidosis but can also be used to evaluate for the presence of acute myocardial infarction or myocarditis. Increased glucose metabolism is considered a hallmark of inflammation due to overexpression of glucose transporters and overproduction of glycolytic enzymes in inflammatory cells.1 In inflammatory processes, PET using the radiolabeled glucose analog 18F-2-deoxy-2-fluoro-D-glucose demonstrates increased uptake in areas of inflammation. The utility of FDG testing is dependent on strict dietary preparation with a high fat and non-carbohydrate diet for 18-24 hours prior to testing in order to suppress normal myocardial glucose uptake.
There is limited data on the utility and efficacy of 18F-FDG PET imaging in detecting pericardial inflammation. Salomaki et al. described the first case showing pericardial inflammation by 18F-FDG PET in 2013 in a patient with postpericardiotomy syndrome.2 PET imaging was initially performed to evaluate for infection and demonstrated strong metabolic activity localizing to the pericardium. Chang et al. found that 18F-FDG pericardial uptake on baseline PET was predictive of steroid responsiveness in a small series of patients with constrictive pericarditis.3 In a recent single center retrospective cohort study of patients admitted for idiopathic acute pericarditis with pericardial effusion, Geradin et al. found that increased FDG pericardial uptake at diagnosis was associated with a higher recurrence rate of pericarditis.4 In this study, only 33% of patients admitted for acute pericarditis with pericardial effusion had pericardial FDG uptake, but no patients in clinical remission had pericardial FDG uptake.4
Echocardiography remains the first-line diagnostic tool for evaluation of pericardial disease.5,6 Cardiac computed tomography (CT) and cardiac magnetic resonance (CMR) remain second-line imaging modalities in the evaluation of pericardial disease and provide better anatomic delineation with cardiac CT useful for evaluating pericardial calcification and CMR helpful in characterizing inflammation.5 The 2015 European Society of Cardiology guidelines for the management of pericardial disease recommend use of PET alone or in combination with CT (PET/CT) to depict the metabolic activity of pericardial disease in select cases but caution that differentiation between physiologic and pathologic cardiac FDG uptake by PET/CT remains challenging.6 A hybrid of 18F-FDG PET and CMR has recently been described in the diagnosis of active pericarditis and may have a future role in pericardial disease.7
Focal and diffuse myocardial FDG uptake patterns (answers A and B) with normal or abnormal perfusion on PET can be seen in cardiac sarcoid, myocarditis and coronary artery disease. In patients with known malignancy, 18F-FDG uptake is indicative of malignant pericardial involvement, and FDG uptake is usually intense and often associated with a focal soft tissue mass (answer C).6 Diffuse pleural FDG uptake (answer E) can be seen in mesothelioma and other pleural diseases.
Unfortunately 18F-FDG PET imaging was negative in this patient. She was treated with colchicine and ibuprofen and ultimately started on steroid-sparing therapy given her young age with an anti-interleukin-1 agent with rapid improvement in her symptoms and inflammatory markers.
References
Kircher M, Lapa C. Novel noninvasive nuclear medicine imaging techniques for cardiac inflammation. Curr Cardiovasc Imaging Rep 2017;10:6.
Salomaki SP, Hohenthal U, Kemppainen J, Pirila L, Saraste A. Visualization of pericarditis by fluorodeoxyglucose PET. Eur Heart J Cardiovasc Imaging 2014;15:291.
Chang SA, Choi JY, Kim EK, et al. [18F]Fluorodeoxyglucose PET/CT predicts response to steroid therapy in constrictive pericarditis. J Am Coll Cardiol 2017;69:750-2.
Gerardin C, Mageau A, Benali K, et al. Increased FDG-PET/CT pericardial uptake identifies acute pericarditis patients at high risk for relapse. Int J Cardiol 2018;271:192-4.
Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr 2013;26:965-1012.
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Xu B, Huang SS, Jellis C, Flamm SD. Diagnosis of active pericarditis by positron emission tomography (PET)/cardiac magnetic resonance (CMR) imaging. Eur Heart J 2018;39:179.