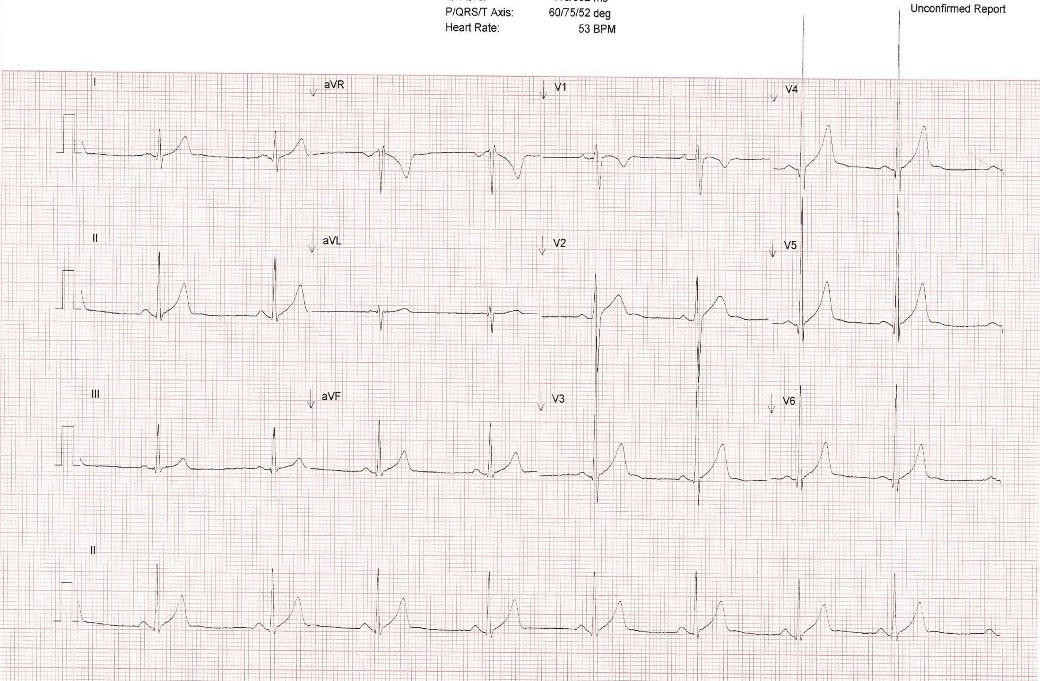
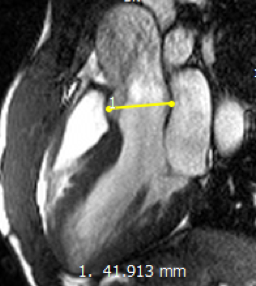
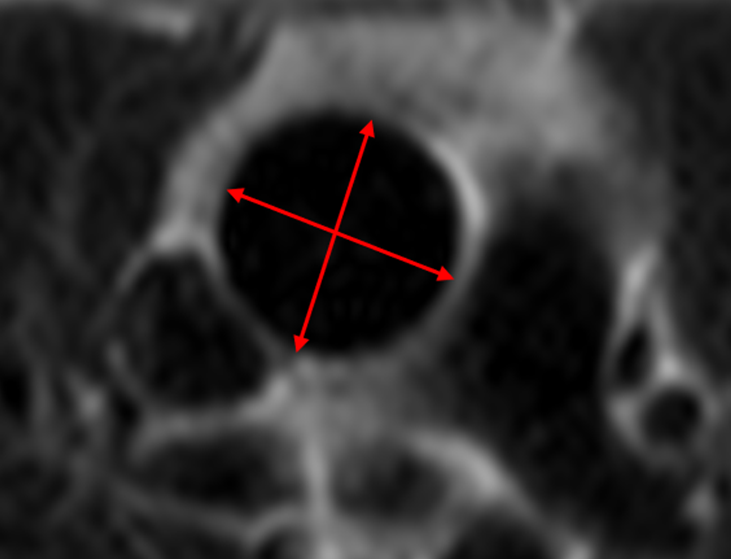
A 20-year-old collegiate American-style football player presents to our sports cardiology clinic after referral from a mobile athletic screening program that included 12-lead electrocardiography and complete 2-D transthoracic echocardiography. He is asymptomatic, has no significant medical history, no significant known family history and takes no medications or supplements. On physical exam, he is 6' tall, weighs 88 kgs, has a blood pressure of 113/72 and has a normal cardiovascular exam with no murmurs or ejection sounds appreciated. He plays as a defensive back, a non-lineman position. His ECG (Figure 1) and selected views from his cardiac imaging studies (Figure 2A and 2B) are shown below. He was found to have a native bicuspid aortic valve and an aortic root with maximum diameter of 42mm by 43 mm as measured by cardiac MRI. There was no aortic stenosis or regurgitation present.
Figure 1: Normal 12-lead electrocardiogram
Figure 1
Figure 2A: CMR With Bicuspid Aortic Valve and No Aortic Stenosis or Regurgitation
Figure 2
Figure 2B: CMR With Maximum Diameter of the Aortic Root (Coronary Sinus) of 42x43mm
Figure 3
According to the 2015 Eligibility and Disqualification Recommendations for Competitive Athletes with Cardiovascular Abnormalities, which of the following is recommended for this condition and specific patient?
Show Answer
The correct answer is: C. At 4.3 cm (aorta), sports such as football are in the exclusion category.
Following the 2015 American Heart Association (AHA) Task Force guidelines, this athlete would be excluded from playing American-style football.1 This document addresses athletes with bicuspid aortic valves (BAV) and includes recommendations based on the severity of aortic dilatation.2 The guidelines differentiate sport type by level of dynamic and static activity, with American-style football classified as a moderate dynamic and static sport (IIB).3 For athletes with a BAV and aorta 43-45mm, the current guidelines allow participation in only low dynamic and static sports (IA). In addition, with a BAV and a dilated aorta in this range the recommendation is to avoid any competitive sports with the potential for bodily collision, such as American-style football.
For athletes with a BAV and moderately dilated aortas measuring 40-42mm, the guidelines allow participation in low and moderate dynamic and static activities, but only those with a low likelihood of body contact. If an athlete with a BAV were found to have an aorta dilated to >45mm, the specific recommendation is to not participate in any competitive sport.2
It is worth noting that the 2015 guidelines utilize the phrases "reasonable" and "might be considered" in line with the Class of Recommendation and Quality of Evidence scheme utilized in contemporary AHA guidelines. This is in contrast to the previous 36th Bethesda Conference guidelines from 2005 which used more absolute terminology, effectively clearing or disqualifying an athlete solely based on the presenting pathology.4 While contemporary guidelines may represent a shift towards ambiguity to some, the lack of binary and absolute branch points now enables physicians to partake in a less paternalistic shared decision-making process with their athletic patients.5 In the case presented, our opinion was that a unilateral disqualification based solely on the guidelines would have been a great disservice to the athlete. The athlete's opinion, his family's opinion and the stance of his school were all vital factors taken into account as part of the final eligibility decision. Studies specifically evaluating the risk of further aortic dilation or dissection as a consequence of ongoing sport participation in patients with bicuspid aortic valves with aortopathy are limited. This paucity of definitive data leads to a reliance on expert consensus, as shown by the Level C evidence for all of the guideline statements in this example. The cultural shift toward shared decision-making allows for the inclusion of a patient's unique situation and individual values to form an arguably more complete and ethical medical evaluation.
References
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities : preamble, principles, and general considerations : a scientific statement from teh American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015 ;66 :2343-9.
Braverman AC, Harris KM, Kovacs RJ, Maron BJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities : task force 7 : aortic diseeases, including Marfan Syndrome : a scientific statement from the American Heart Association and the American College of Cardiology. J Am Coll Cardiol 2015 ;66 :2398-405.
Levine BD, Baggish AL, Kovacs RJ, Link MS, Maron MS, Mitchell JH. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities : task force 1 : classification of sports : dynamic, static, and impact : a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015 ;66 :2350-5.
Maron BJ, Zipes DP. Introduction : eligibility recommendations for competitive athletes with cardiovascular abnormalities-general considerations. J Am Coll Cardiol 2005 ;45 :1318-21.
Baggish AL, Ackerman MJ, Lampert R. Competitive sport participation among athletes with heart disease : a call for a paradigm shift in decision making. Circulation 2017 ;136 :1569-71.