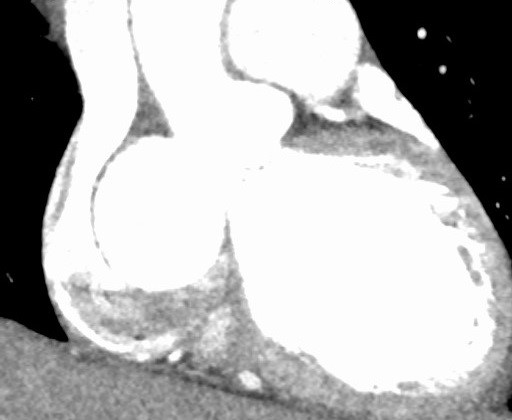
A 52-year-old female patient with a history of seizures and hypertension presents to urgent care with a pre-syncopal episode of dizziness and hypotension. She has no history of dizziness unrelated to seizures. This episode occurred at work with no heavy lifting or new activity. She does not report chest pain, shortness of breath, nausea, fever, chills or vomiting. The patient reports a recent cold that is getting better. She has no surgical history. An electrocardiogram, troponin levels, and chest X-ray are all normal. She underwent computed tomography (CT) imaging with contrast pulmonary embolism (PE) protocol at the urgent care facility that was negative for PE, but what was found in Figure 1 prompted transfer to a tertiary center. On your exam in the emergency room, you confirm the patient's story. On physical exam, the only abnormality you note is on auscultation of the heart, where you find a 4/6 mid diastolic blowing murmur in the aortic foci and apex that radiates to the axilla.
Figure 1
Figure 1
Which of the following is the best way to proceed with this patient?
Show Answer
The correct answer is: B. Echocardiogram and CT angiogram of chest
With unknown cardiac masses, the best approach to diagnosis is better definition of anatomy. In this case, this was done via a transthoracic echocardiogram and CT angiogram of chest. Two-dimensional echocardiography is often adequate to assess cardiac mass within all four chambers, and color flow can identify the etiology of a murmur. Use of electrocardiogram-gated CT angiography can further define cardiac anatomy (Figures 2-3).
Figure 2
Figure 2
Figure 3
Figure 3
Sinus of Valsalva aneurysms account for 0.1-3.5% of all congenital heart defects and are encountered in 0.14-0.96% of open-heart surgery cases.1Sinus of Valsalva is defined as an abnormal dilation of the aortic root located between the aortic valve annulus and the sinotubular ridge. Unruptured sinus of Valsalva is usually asymptomatic; however, patients may experience exertional dyspnea, palpitations, and angina-like chest pain.2 Sinus of Valsalva is usually diagnosed in the setting of a rupture. In that setting, the left-to-right shunting produces acute dyspnea and chest pain in one-third of patients. Half of the patients note gradually worsening dyspnea, fatigue, chest pain, and peripheral edema, and the remainder of patients is asymptomatic.3
Clinical signs that should lead to a high suspicion of sinus of Valsalva are a continuous murmur heard best along the left sternal border from the second to the fourth intercostal space with a diastolic accentuation, which may help differentiate ruptured sinus of Valsalva from patent ductus arteriosus, and a low diastolic blood pressure. On two-dimensional echocardiography, asymmetric dilatation of the aortic root can be visualized. With Doppler, a color jet from the aortic root into the right atrium or ventricle, diastolic opening of the pulmonary valve and fluttering of the tricuspid valve leaflets may be seen.4
If a ruptured sinus of Valsalva is identified, surgical correction is indicated on an emergency basis because early treatment can reduce the risk of infective endocarditis, the development of congestive heart failure, and mortality. Surgical treatment consists of closure of the fistulous tract with autologous or bovine pericardium, with or without aortic valve replacement or repair.5
Our patient had a sinus of Valsalva aneurysm with severe aortic regurgitation due to aortic root enlargement up to 7 cm. The patient underwent repair of her noncoronary sinus of Valsalva aneurysm by performing the Bentall procedure using a 27 mm Valsalva mechanical valve conduit. This was not ruptured, so there was no fistulous connection. Our patient did well and was home within 5 days.
References
Fishbein MC, Obma R, Roberts WC. Unruptured sinus of Valsalva aneurysm. Am J Cardiol 1975;35:918-22.
Heydorn WH, Nelson WP, Fitterer JD, Floyd GD, Strevey TE. Congenital aneurysm of the sinus of Valsalva protruding into the left ventricle. Review of diagnosis and treatment of the unruptured aneurysm. J Thorac Cardiovasc Surg 1976;71:839-45.
Bonfils-Roberts EA, DuShane JW, McGoon DC, Danielson GK. Aortic sinus fistula--surgical considerations and results of operation. Ann Thorac Surg 1971;12:492-502.
Arıkan E, Karagöz A, Bayata S, Yilik L, Unlüer EE. A rare cause of dyspnea: sudden rupture of aortic valsalva sinus aneurysm. Case Rep Med 2013;2013:909302.
Encarnacion CO, Loranger M, Bharatkumar AG, Almassi GH. Bacterial Endocarditis Caused by Lactobacillus acidophilus Leading to Rupture of Sinus of Valsalva Aneurysm. Tex Heart Inst J 2016;43:161-4.