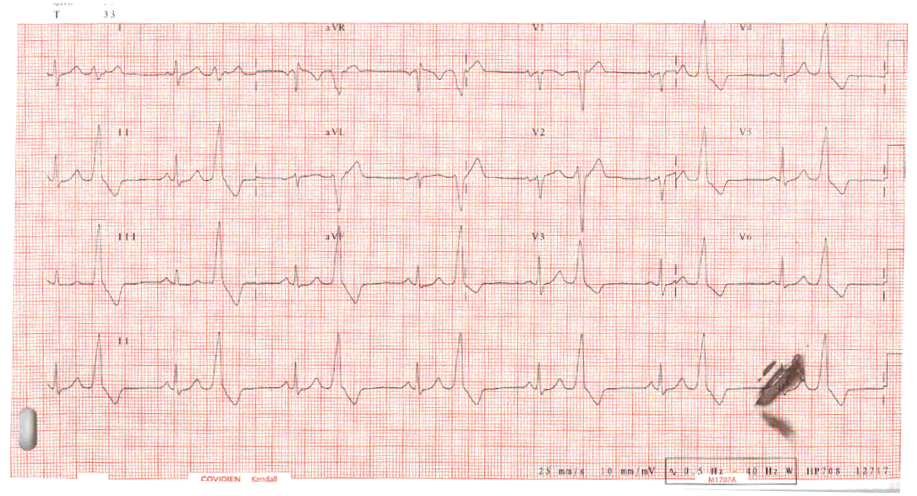
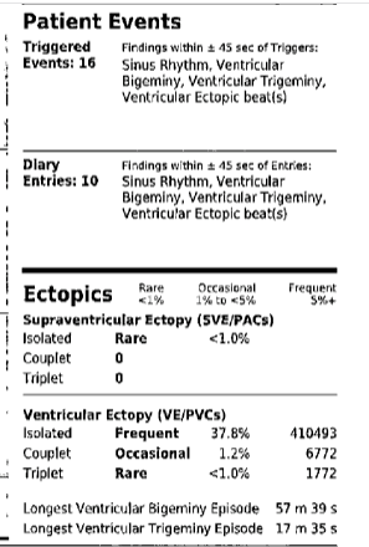
A 23-year-old male lacrosse player with no significant medical history reported having new onset palpitations while standing on the sideline at practice. He denied shortness of breath, chest pain, or pre-syncope. He denied any stimulant use. He had no family history of arrhythmia, arrhythmogenic right ventricular cardiomyopathy(ARVC), premature cardiovascular disease, or sudden unexplained death. Physical examination was grossly normal except for premature beats on auscultation. Electrocardiogram, shown in Figure 1, was consistent with sinus rhythm and ventricular bigeminy. The premature ventricular contractions (PVCs) were monomorphic with a left bundle branch (LBBB) pattern and inferior axis suggestive of focal right ventricular outflow tract (RVOT) origin. No epsilon waves were noted. The patient was given a Holter monitor which showed a 35% PVC burden as well as sustained episodes of both bigeminy and trigeminy (Figure 2). He reported feeling palpitations that corresponded with runs of ectopic beats. A high-quality echocardiogram was performed which showed preserved biventricular size and function as well as normal valvular function. In particular, the right ventricle was well visualized and did not demonstrate any abnormalities.
Figure 1: Initial ECG
Figure 1
Figure 2: Holter Monitor Results
Figure 2
What is the most appropriate step in the management of this patient?
Show Answer
The correct answer is: F. Electrophysiology (EP) study with possible catheter ablation
This 23-year-old previously healthy lacrosse player with a structurally normal heart was found to have symptomatic PVCs. His PVC burden was found to be >35% and were in a pattern suggestive of RVOT origin (LBBB, inferior axis). While a cardiac MRI is not unreasonable, this individual had a high quality, normal echocardiogram with good visualization of the RV and no symptoms suggestive of cardiomyopathy. If he had PVCs of a non-outflow tract origin, or had multifocal PVCs, an MRI would be a reasonable next step to evaluate his myocardium and rule out ARVC. An exercise treadmill test is not necessary since symptoms and PVCs were documented at rest. Initiating Amiodarone in such a young patient would put him at risk for significant side effects and therefore not a reasonable long-term strategy. Beta blockers tend to not be very effective at suppressing PVCs. Moreover, high performance athletes tend to not tolerate beta blockers very well due to blunting of heart rate response.
A trial of Flecainide could be considered, but again would not be ideal in such a young patient. Interestingly, a study published this year found that Flecainide was both effective and well tolerated in patients with PVC induced cardiomyopathy.1
Thus, we concluded that an EP study with possible PVC ablation would be most appropriate.
In a study of over 5000 athletes, a small cohort (n=36, 0.7%) had a high burden of PVC's (at least 10 PVCs, ≥1 ventricular couplet, ≥1 burst of non-sustained ventricular tachycardia) during stress testing.2 Six in total underwent radiofrequency (RF) ablation (five in the RVOT). All six who underwent ablation had significant enough reduction in PVCs and resolution of symptoms to return to competition. It is important to note that 23 of the patients in this study spontaneously recovered and returned to competition without intervention over the following 3-12-month period. A second study from that same year showed that PVC ablation was both safe and highly successful (71% at 2 years without the use of antiarrhythmics). Furthermore, ablation was shown to be safe (complication rate of 5.2%) even in patients with high PVC burden as well as those with PVC induced cardiomyopathy. In fact, patients with PVC induced cardiomyopathy (CM) saw a significant increase in ejection fraction (EF) after ablation procedure.3 Knowing the above information, it would not be unreasonable to consider a "watch and wait" approach that included detraining (if the athlete is agreeable), especially in the context of a structurally normal heart. Given the success rate of RVOT PVC ablations, the patient's significant symptomology and his desire to return to competition quickly, a joint decision was made to proceed with ablation with the hope of rapid and sustained resolution.
At 3 month follow up, a 14-day ECG monitor showed no PVCs. He remained symptom free and returned to lacrosse.
References
Hyman MC, Mustin D, Supple G et al. Class IC antiarrhythmic drugs for suspected premature ventricular contraction-induced cardiomyopathy. Heart Rhythm 2018;15:159-63.
Verdile L, Maron BJ2, Pelliccia A, Spataro A, Santini M, Biffi A. Clinical significance of exercise-induced ventricular tachyarrhythmias in trained athletes without cardiovascular abnormalities. Heart Rhythm 2015;12:78-85.
Latchamsetty R, Yokokawa M, Morady F et al. Multicenter outcome for catheter ablation of idiopathic premature ventricular complexes. JACC Clin Electrophysiol 2015;1:116-23.