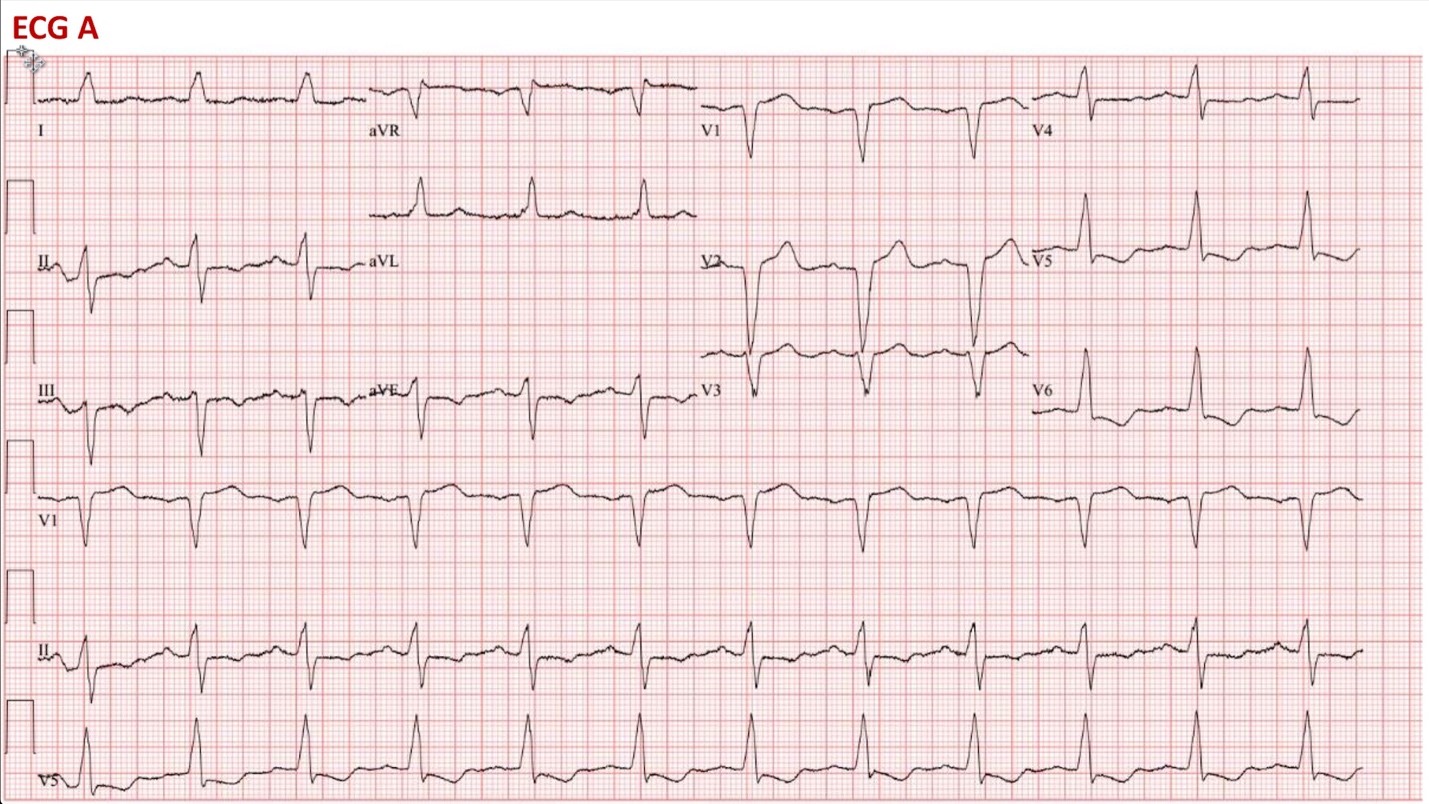
A 79-year-old woman with a history of severe aortic stenosis after transcatheter aortic valve replacement (TAVR), coronary artery disease with previous percutaneous coronary intervention (PCI), hypertension, dyslipidemia, and left bundle branch block (LBBB) presents to outpatient clinic with near syncope. One week prior to presentation she underwent uncomplicated TAVR with placement of a 26mm Edwards SAPIEN 3 balloon expandable valve. Her pre-TAVR ECG (ECG A) shows sinus rhythm with LBBB. A second ECG (ECG B) was performed at the time of her clinic visit:
ECG A
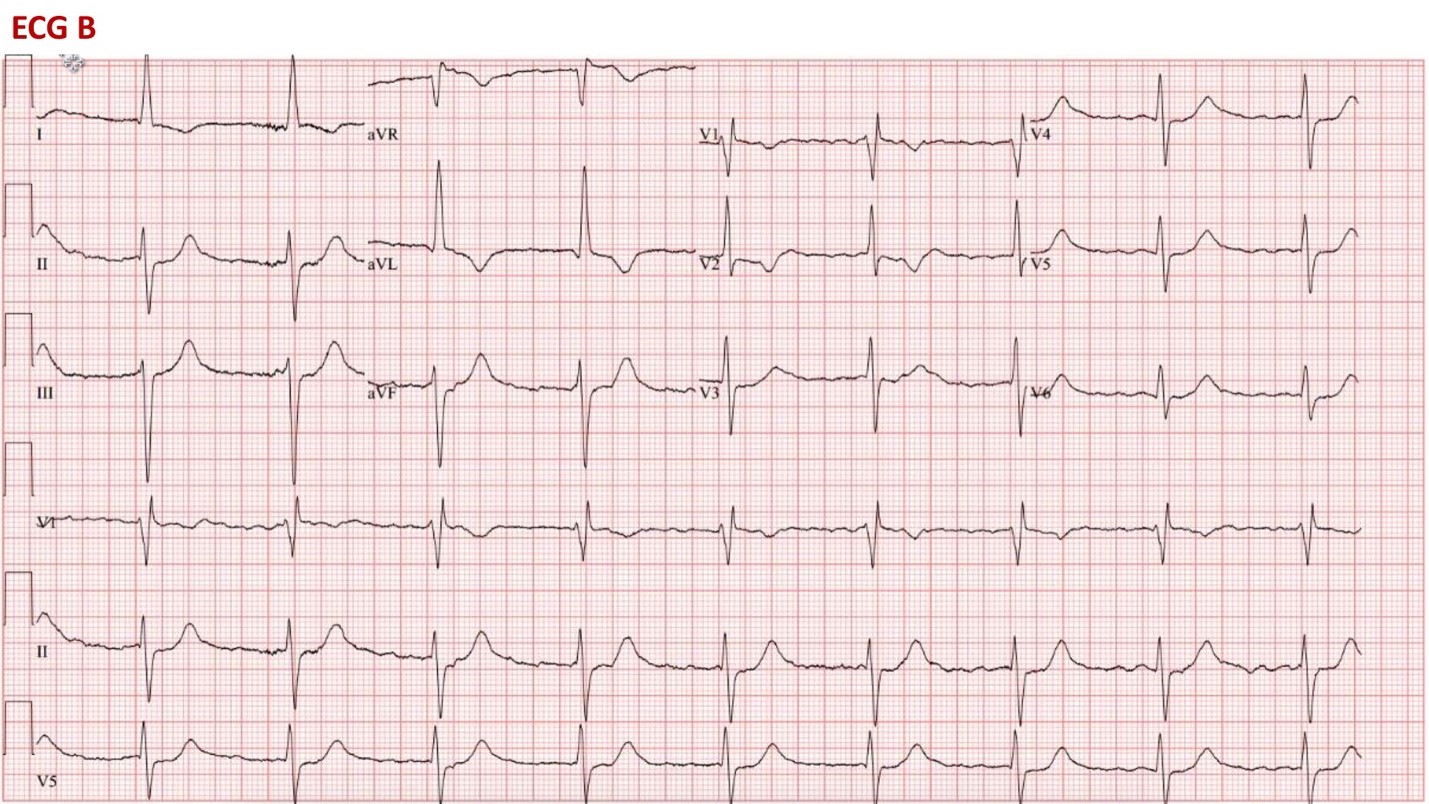
ECG B
ECG B shows which of the following:
Show Answer
The correct answer is: B. Atrial fibrillation with complete AV block.
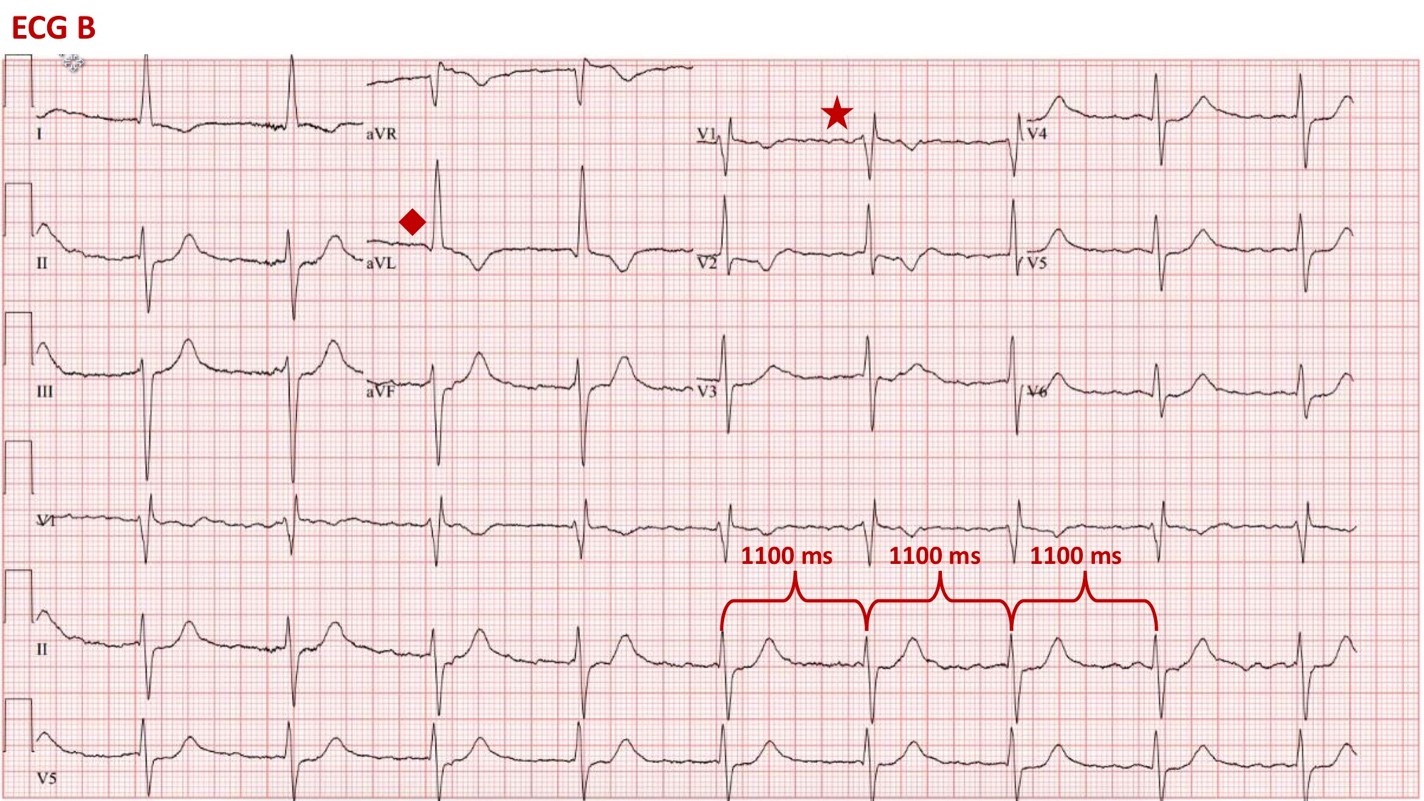
The underlying rhythm of ECG B is atrial fibrillation with complete heart block and a junctional escape rhythm at a rate of 55 bpm. There is a clear absence of P waves consistent with atrial fibrillation; however, the R-R interval is regular (1100ms), indicating that there is complete dissociation of the atria and ventricles, consistent with an underlying junctional escape rhythm. Additionally, she now demonstrates a new conduction abnormality, with both a right bundle branch block (note the characteristic RSR' in V1 [red star]), and a left anterior fascicular block demonstrated by the presence of left axis deviation (greater than -45 degrees) and qR complex in aVL (red diamond). Given the presence of atrial fibrillation with complete heart block, a pacemaker was indicated. Additionally, she has now demonstrated alternating bundle branch block, a situation where block all three fascicles (RBBB, LAFB, and LPFB) are demonstrated on successive ECGs. In our patient we have evidence of conduction system disease initially involving the left bundle branch (ECG A), and subsequently the right bundle branch (ECG B). Her alternating bundle branch block alone may warrant pacemaker even if she were in sinus rhythm, as these patients often progress rapidly to complete AV block.1 She was admitted and underwent successful placement of a dual-chamber pacemaker.
ECG B
There is no evidence of organized atrial activity in ECG B, therefore answers A and D are incorrect. Idioventricular rhythm does not occurs with atrial fibrillation and has wider QRS duration without RBBB morphology, therefore answer C is not correct.
Complete heart block and worsening of conduction abnormalities are common complications following TAVR.1 Predictors of advanced conduction disturbance including complete heart block requiring permanent pacemaker (PPM) placement post TAVR include pre-existing conduction abnormalities, new conduction abnormalities at time of implantation, larger prosthesis size, valve oversizing, increased implantation depth and use of a self-expanding valve.2,3
References
Brignole M, Auricchio A, Baron-Esquivas G, et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on Cardiac Pacing and Resynchronization Therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J 2013;34:2281-329.
Fadahunsi OO, Olowoyeye A, Ukaigwe A, et al. Incidence, predictors, and outcomes of permanent pacemaker implantation following transcatheter aortic valve replacement: analysis from the U.S. Society of Thoracic Surgeons/American College of Cardiology TVT Registry. JACC Cardiovasc Interv 2016;9:2189-99.
Mangieri A, Lanzillo G, Bertoldi L, et al. Predictors of advanced conduction disturbances requiring a late (≥48 H) permanent pacemaker following transcatheter aortic valve replacement. JACC Cardiovasc Interv 2018;11:1519-26.