A 30-year-old G1P1 female with a past medical history significant for fibrosing mediastinitis secondary to pulmonary histoplasmosis (treated with itraconazole in 2015) and acute pericarditis presents to cardiology clinic for a follow-up visit. She was diagnosed with acute pericarditis approximately two months prior to going into labor after complaining to her family physician of persistent pleuritic chest pain. Given that she was pregnant, she was initially prescribed single therapy of prednisone 20 mg daily and her symptoms subsided shortly thereafter. However, 2 months after her initial diagnosis she re-presented with chest discomfort and a large pericardial effusion that required drainage after an emergent delivery. Post-partum, she has been treated with ibuprofen and colchicine.
She presents today, four weeks after delivery, with ongoing symptoms. She remains on ibuprofen and colchicine. She reports worsening dyspnea, especially on exertion. Furthermore, she endorses chest pain that is worse in the supine position. Her inflammatory markers reveal a sedimentation rate of 38 mm/hr [normal 0 - 20 mm/hr] and an ultra-sensitive C-reactive protein level of 51.6 mg/L [normal <3.1 mg/L]. Her ECG is shown in Figure 1, and previous echocardiogram in Figures 2 and 3. A cardiac magnetic resonance imaging (MRI) was ordered to further assess the pericardium and pericardial effusion.
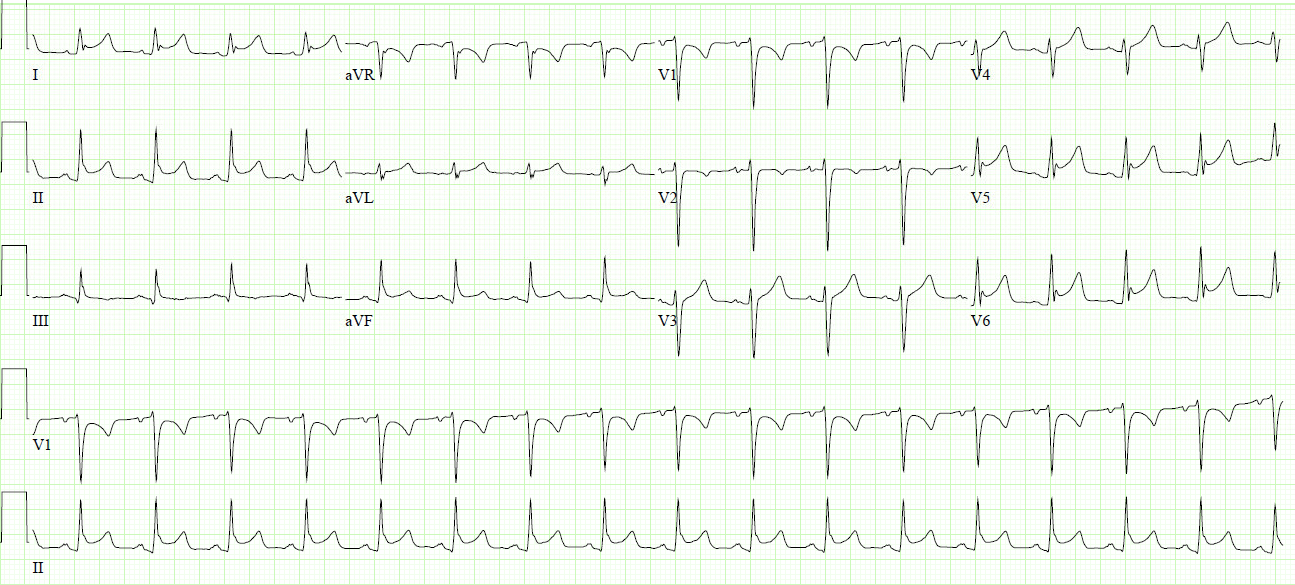
Figure 1
Figure 1
Figure 1: Electrocardiogram displaying ST elevations in multiple leads, PR elevation in aVR and, PR depressions in I, II, aVF, and V3-V6 in a pattern consistent with pericarditis.
Figure 1: Electrocardiogram displaying ST elevations in multiple leads, PR elevation in aVR and, PR depressions in I, II, aVF, and V3-V6 in a pattern consistent with pericarditis.
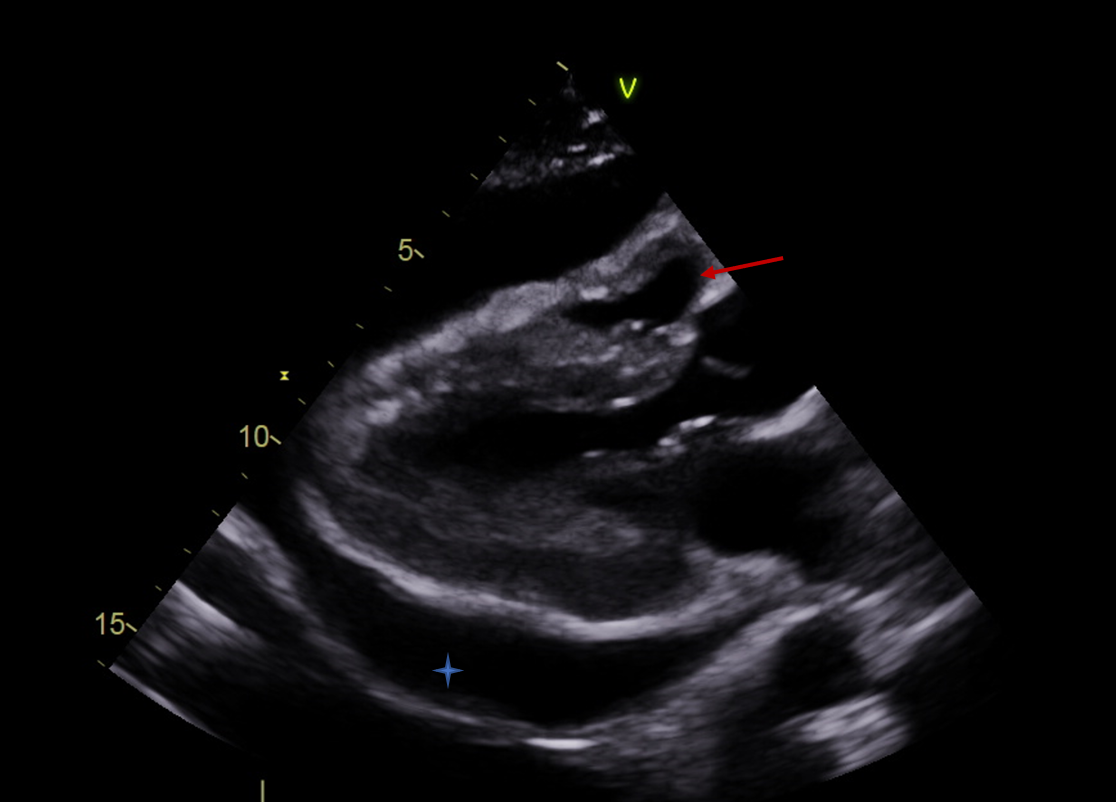
Her echo (below) from four weeks ago reveals the large circumferential pericardial effusion with tamponade features that required pericardiocentesis at the time.
Figure 2
Figure 2
Figure 2: Parasternal long-axis view revealing almost complete collapse of the right ventricle (red arrow) due to large circumferential pericardial effusion (*)
Figure 2: Parasternal long-axis view revealing almost complete collapse of the right ventricle (red arrow) due to large circumferential pericardial effusion (*)
Figure 3
Figure 3
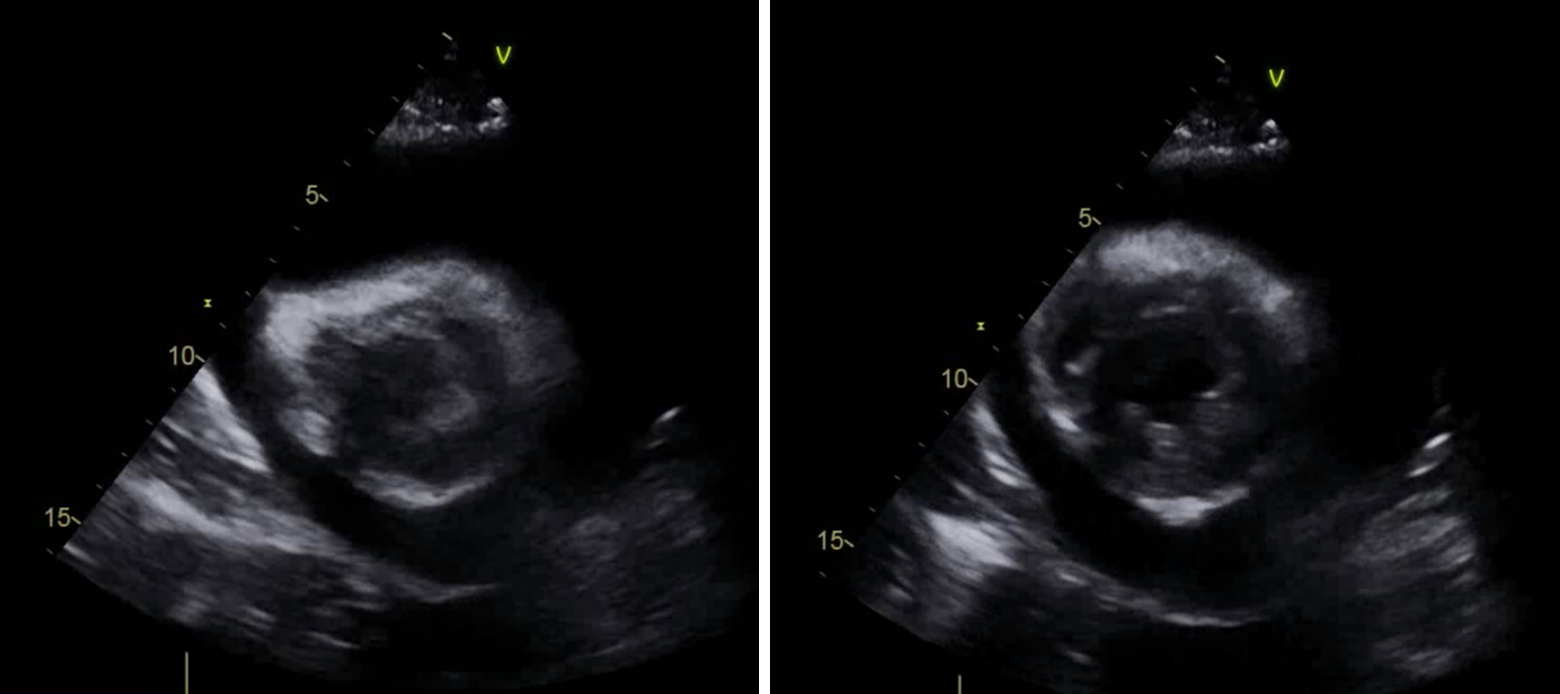
Figure 3: Parasternal short-axis view during systole (left) and diastole (right) revealing little or no diastolic expansion of the right ventricle.
Figure 3: Parasternal short-axis view during systole (left) and diastole (right) revealing little or no diastolic expansion of the right ventricle.
Figure 4
Figure 4
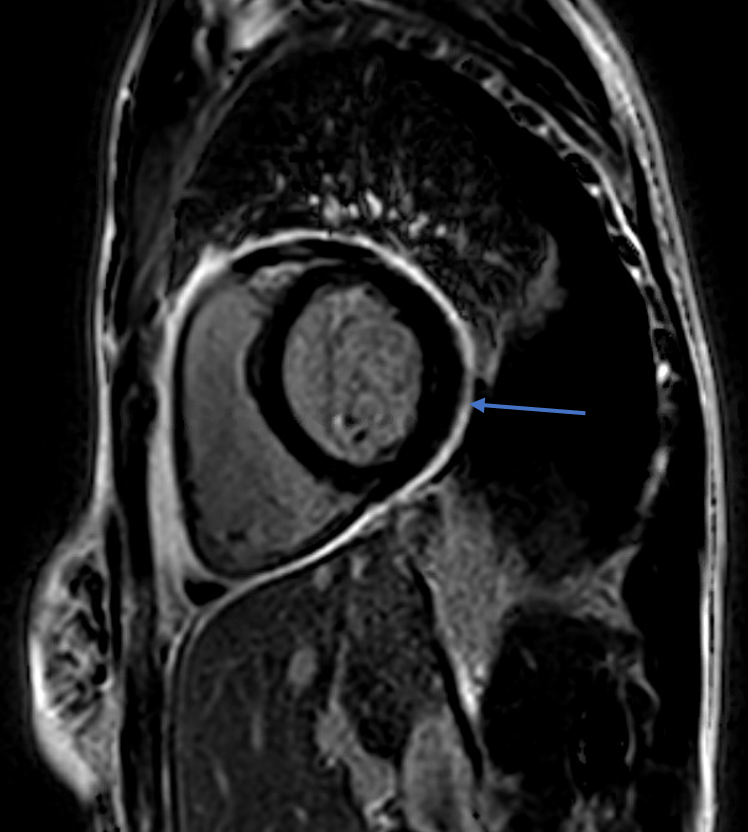
Figure 4: Cardiac MRI (on day of office visit) delayed sequence after gadolinium injection revealing mild pericardial thickening, and qualitatively moderate circumferential increased pericardial delayed enhancement (arrow).
Figure 4: Cardiac MRI (on day of office visit) delayed sequence after gadolinium injection revealing mild pericardial thickening, and qualitatively moderate circumferential increased pericardial delayed enhancement (arrow).
Review of her inpatient computed tomography (CT) chest revealed calcified mediastinal and right hilar lymph nodes in keeping with her history of fibrosing mediastinitis.
Out of concern for reactivation of pulmonary histoplasmosis, infectious disease specialists decide to start the patient on an anti-microbial. She is four weeks post-partum and would like to begin breastfeeding. She is worried about taking these medications while breastfeeding.
What is the best course of action in regards to her treatment regimen?
Show Answer
The correct answer is: B. Add prednisone to her current regimen of ibuprofen and colchicine
It was thought that the patient's pericarditis was triggered by an underlying histoplasmosis infection. Between 5-10% of pulmonary histoplasmosis develop pericarditis.1-3 Pericardial fluid analysis from our patient's pericardiocentesis four weeks prior was not suggestive of an infection. However, with regards to pericarditis, pulmonary histoplasmosis typically elicits an inflammatory process, rather than an infectious one.3
The patient's ongoing symptoms, findings on clinical examination, ECG, inflammatory markers, and imaging, suggest that her presentation is most consistent with active incessant pericarditis. Her cardiac MRI showed a thickened pericardium with associated delayed gadolinium enhancement, establishing that this is an ongoing recurrence that will likely require an aggressive and protracted treatment course.4 Low-dose prednisone was an appropriate therapy during her pregnancy, as it is the recommended treatment for a pregnant patient after 20 weeks gestation.5 As noted, prednisone was switched to anti-inflammatory agents (ibuprofen and colchicine) at adequate doses post-partum. However, since her symptoms have been ongoing since her recurrence began four weeks ago, she has proven to have failed her current therapy. Therefore, choice A would be incorrect as her clinical course would suggest this regimen is not sufficient.
When there is an incomplete response to aspirin/NSAIDs and colchicine, recurrent pericarditis typically requires another agent, i.e. corticosteroids. The patient's concerns are well-founded as treatment of pericarditis during pregnancy is limited by the agents available and the weeks of gestation. Aspirin/NSAIDs are typically avoided after twenty weeks of gestation out of concern for risk of premature closure of the ductus arteriosus in the fetus, while colchicine is avoided completely throughout pregnancy.5
The safety of colchicine during breastfeeding has already been studied in Familial Mediterranean Fever (FMF). Several studies have shown that colchicine does indeed present in the breast milk at trace concentrations.6,7 The concentration of colchicine in the mother's serum and breastmilk were found to be similar at different time points in a 24-hour period. However, it is estimated that the total daily ingestion of colchicine through breast milk is one-tenth the amount an adult is exposed to in the same period. Clinical follow-up over ten months to two years showed no apparent clinical or developmental effects on the children.7 Of note, these patients were taking colchicine at doses comparable to the dose used in the treatment of pericarditis, 1-1.5 mg daily. Therefore, it was deemed that colchicine was safe to use during breastfeeding. The American Academy of Pediatrics Committee on Drugs noted in 2001 that there is no noted clinical effect of colchicine on the infant while breastfeeding, while also noting that data is limited to a small series of infants. In 2015, a prospective observational cohort study found no increase in adverse long-term outcomes in colchicine-exposed breastfed children when compared to breastfed infants not exposed to colchicine.8 The European Society of Cardiology (ESC) guidelines on pericarditis in 2015 noted that colchicine is considered to be contraindicated in breastfeeding, though the same guidelines state that no adverse events have been noted in children who are breastfed from women with FMF treated with colchicine.5
Therefore, holding colchicine (choice C) would be incorrect as it is part of the treatment regimen for recurrent pericarditis. The correct answer would be B. Use of a corticosteroid-sparing agent (choice D) would be warranted after failure of prednisone in addition to her current regimen. Exercise restriction to keep her heart rate to prevent excessive tachycardia may also be warranted. Lastly, as with all medications in the peripartum period, medication initiations and modifications should only be after a discussion with the patient and primary obstetrics specialist.
References
Wheat LJ, Slama TG, Eitzen HE, Kohler RB, French ML, Biesecker JL. A large urban outbreak of histoplasmosis: clinical features. Ann Intern Med 1981;94:331–37.
Wheat LJ, Stein L, Corya BC, et al. Pericarditis as a manifestation of histoplasmosis during two large urban outbreaks. Medicine 1983;62:110–19.
Wang JJ, Reimold SC. Chest pain resulting from histoplasmosis pericarditis: a brief report and review of the literature. Cardiol Rev 2006;14:223–26.
Kumar A, Sato K, Verma BR, et al. Quantitative assessment of pericardial delayed hyperenhancement helps identify patients with ongoing recurrences of pericarditis. Open Heart 2018;5:e000944.
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Milunsky JM. Breast feeding during colchicine therapy for familial Mediterranean fever. J Pediatr 1991;119:164.
Ben-Chetrit E, Scherrmann JM, Levy M. Colchicine in breast milk of patients with familial Mediterranean fever. Arthritis Rheum 1996;39:1213-17.
Herscovici T, Merlob P, Stahl B, Laron-kenet T, Klinger G. Colchicine use during breastfeeding. Breastfeed Med 2015;10:92-5.