A 60-year-old male with prior history of mediastinal radiation for treatment of Hodgkin's lymphoma, coronary artery disease (CAD), bioprosthetic aortic and mitral valve replacement, and paroxysmal atrial fibrillation presented to clinic with exertional dyspnea. His symptoms have been ongoing for 6 months along with abdominal distention, weight gain of 24 pounds and lower extremity swelling. He has recently noticed a decline in his exercise tolerance. He denied chest pain, orthopnea or paroxysmal nocturnal dyspnea. His cardiac history is significant for right coronary artery (RCA) drug-eluting stent (DES) insertion and aortic and mitral valve replacements with 23 mm and 29 mm bioprosthetic valves respectively (a year ago). He was recently started on prednisone 40 mg daily for possible constrictive pericarditis due to post-pericardiotomy syndrome. Patient developed acute kidney injury previously with use of ibuprofen and was unable to tolerate colchicine. His other medications were aspirin, clopidogrel, carvedilol, warfarin, digoxin, furosemide, and pitavastatin.
On physical exam he was afebrile with a blood pressure of 134/68 mmHg, pulse 74/min, respiratory rate 12/min, saturating 98% on room air. He appeared comfortable at rest. He had an elevated jugular venous pressure (8cm H2O), regular heart rhythm, holosystolic murmur over the left lower sternal border, diminished basal lung sounds, distended abdomen, and 1+ pitting edema of the bilateral lower extremities. Serum creatinine was 1.5 mg/dl [normal range: 0.58-0.96 mg/dL], which was at his baseline. Erythrocyte sedimentation rate (ESR) was 12 mm/hr [normal range: 0-15 mm/hr], ultra-sensitive C-reactive protein (us-CRP) was elevated at 8.1 mg/L [normal range: <3.1mg/L), NT pro-BNP was elevated at 899 pg/mL [normal range: <125pg/mL). Complete blood count, liver function tests, electrolyte panel and urinalysis were unremarkable. Electrocardiogram showed normal sinus rhythm with first-degree atrioventricular block (PR interval 284 milliseconds) without any ST elevation or PR depression.
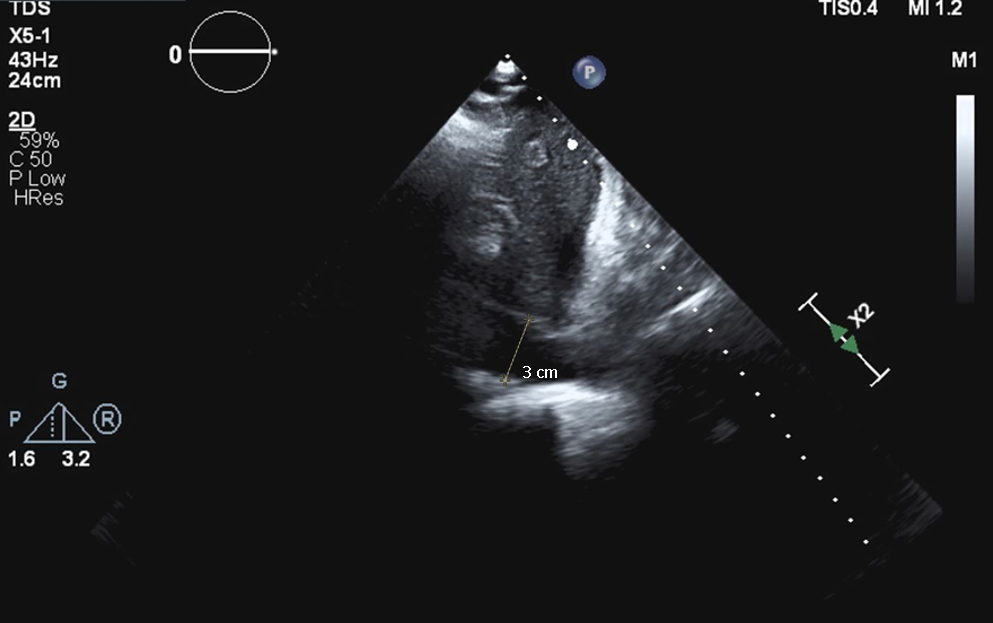
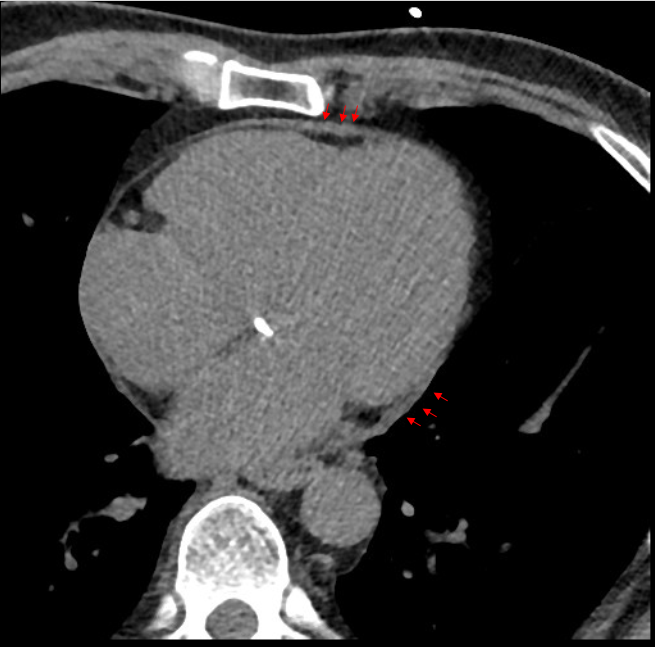
The patient underwent transthoracic echocardiogram which showed normal left ventricular size and ejection fraction of 60%, mildly decreased right ventricular systolic function and moderate tricuspid regurgitation. Also showed tethering of the right atrial and right ventricular free wall, dilated inferior vena cava (3 cm), respirophasic septal shift, medial e' velocity of 5 cm/s, and hepatic vein expiratory diastolic reversal velocity ratio of 1.08. Prosthetic aortic and mitral valves were normally functioning (Image 1). Gated computerized tomography (CT) scan of the chest showed a thickened pericardium (Image 2). Cardiac magnetic resonance (CMR) imaging showed tubular/conical ventricular deformities, septal bounce, mild abrupt cessation of diastolic filling and prominent respirophasic septal shift on free breathing sequence (Video 1). On delayed enhancement imaging there was no pericardial late gadolinium enhancement or increased pericardial signal intensity to suggest pericardial inflammation/active pericarditis. A dual-transducer constriction study showed elevated right and left sided filling pressures with equalization of diastolic pressures, but concordant changes in right and left ventricular systolic pressures during inspiration. Systolic area index was not calculated (Table 1).
Image 1A
Image 1A
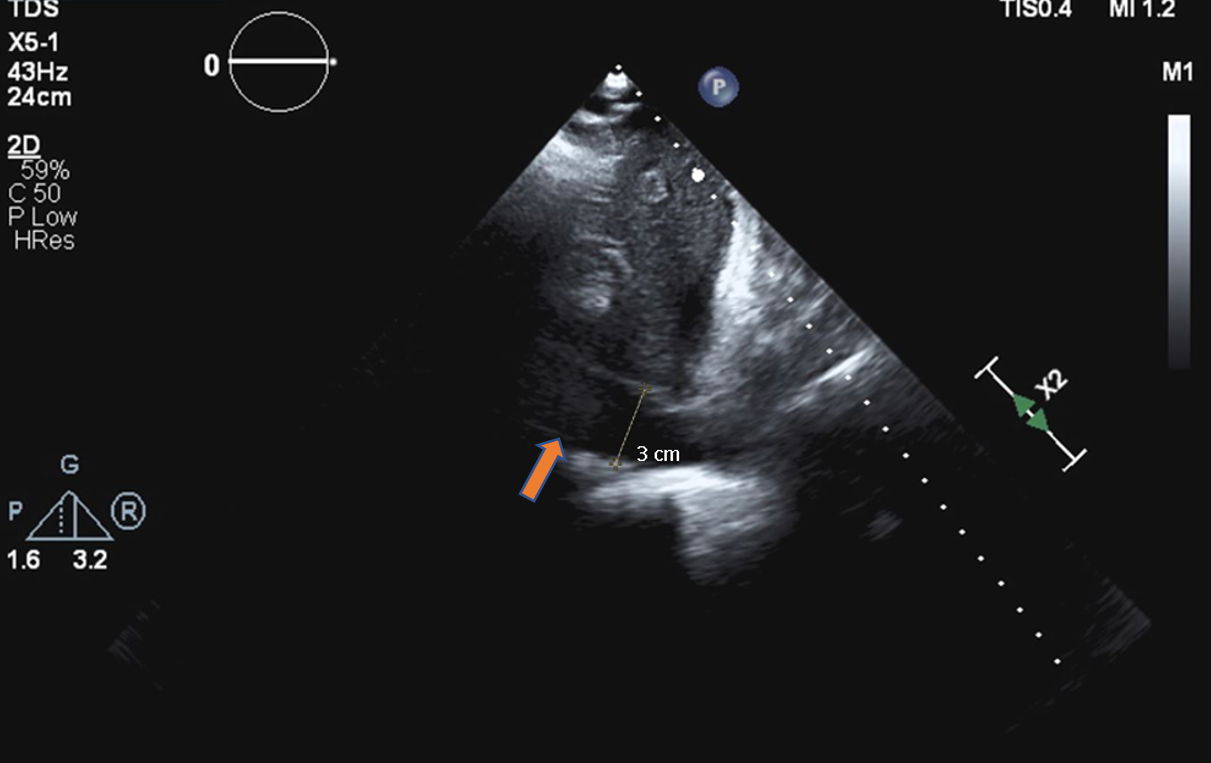
Image 1A: Transthoracic echocardiography subxiphoid view of the inferior vena cava (3 cm).
Image 1A: Transthoracic echocardiography subxiphoid view of the inferior vena cava (3 cm).
Image 2A
Image 2A
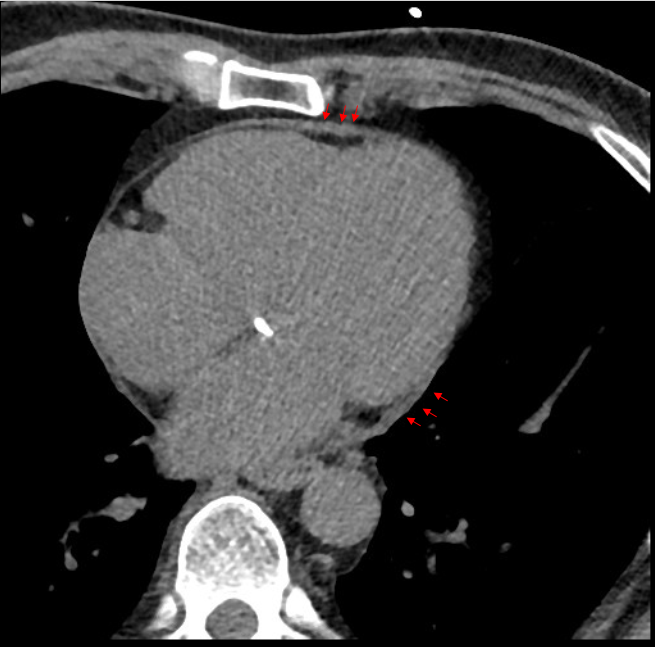
Image 2A: Non-contrast gated computerized tomographic image of the chest with reconstructed 4-chamber view demonstrating increased pericardial thickness (red arrows).
Image 2A: Non-contrast gated computerized tomographic image of the chest with reconstructed 4-chamber view demonstrating increased pericardial thickness (red arrows).
Video 1A
Video 1A
Video 1A: Cardiac magnetic resonance imaging free breathing cine sequence.
Video 1A: Cardiac magnetic resonance imaging free breathing cine sequence.
Table 1A: Pressure recordings from cardiac catheterization of right atrium, ventricle, left atrium and left ventricle.
What is the most likely diagnosis?
Show Answer
The correct answer is: E. Mixed heart disease (constriction and restrictive cardiomyopathy)
Constrictive pericarditis (CP) and restrictive cardiomyopathy are two important etiologies to consider in the differential diagnosis in patients with symptoms of heart failure with preserved left ventricular ejection fraction. Differentiating between these two can sometimes be difficult but clinically it is very important. This is because constrictive pericarditis is treated surgically with pericardiectomy while restrictive cardiomyopathy requires optimized medical regimen. CMR and cardiac catheterization have an essential role in providing anatomical and pathophysiological data to guide the diagnostic evaluation.1 However, in our case imaging features of both conditions are present hence the correct answer is mixed heart disease – pericardial constriction and restrictive cardiomyopathy.
Based on literature review, there has been a rise in the "frequency" of constrictive pericarditis patients due to prior cardiac surgery or radiation therapy.2 Radiation therapy to the chest, particularly mediastinal, is a known risk factor for constrictive pericarditis as well as restrictive cardiomyopathy. Hemodynamically, cardiac filling is impaired in constrictive pericarditis due to abnormal pericardial restraint while in restrictive cardiomyopathy diastolic filling is impaired due to impaired ventricular relaxation. To distinguish these conditions, investigations include an echocardiogram, CT scan, CMR and/or cardiac catheterization.
Echocardiogram is usually the first line of imaging which provides hemodynamic as well as structural information. Based on the criteria used by the Mayo Clinic, presence of ventricular septal shift, medial mitral e' and hepatic vein expiratory diastolic reversal ratio have 97% specificity and 64% sensitivity to diagnose constrictive pericarditis. Medial e` velocity >9 cm/s alone has specificity and sensitivity of 81% and 83% respectively.3 However, in our case, due to prior mitral valve replacement, the medial mitral e` could not be assessed for diagnostic purposes. In patients with restrictive cardiomyopathy, echocardiography usually reveals small left ventricles along with biatrial enlargement, E/A ratio >2, no significant respiratory variations across mitral valve and tissue Doppler peak e`<8 cm/sec.1
In patients with CP, a CT scan can reveal a thickened pericardium (>2 mm), however in ~18% cases it may be normal.4 CT can also detect pericardial calcification and provides assessment of the cardiac structures to guide the peri-operative approach (especially in re-do open heart surgeries). It is especially helpful when echocardiogram is non-conclusive or if patient is unable to undergo CMR. On gadolinium delayed enhanced cardiac CMR imaging, the presence of pericardial late gadolinium enhancement (LGE) represents ongoing inflammation and can be a reliable indicator of response to anti-inflammatory therapy.5-7 However, in our case LGE was not present suggesting the absence of ongoing pericarditis due which anti-inflammatory therapy may not provide any benefit.1 CMR in patients with CP provides both structural and hemodynamic data with 93% diagnostic accuracy based on criteria such as: respirophasic discordance in atrioventricular valve inflow velocity variation, septal shift, pericardial thickness (>4 mm), diastolic septal bounce, and plethoric inferior vena cava (Table 2).8
Table 2
CONSTRICTION
RESTRICTION
Clinical
History of radiation
Present
Present
History of connective tissue disorder
Present
Present
Jugular venous pressure - y
⇑
⇑
Jugular venous pressure - x
⇑
⇓
Kussmaul's sign
Present
Present
Advanced Cardiac Imaging findings
Echocardiography
Medial e' velocity >9cm/s
Present
Absent
Medial e'/lateral e' >0.91
Present
Absent
Hepatic veins
Forward velocity is
Diastolic reversals
Decreased
Increased
Increased expiratory
Increased inspiratory
Trans-valvular flow
Mitral
Tricuspid
>25% expiratory increase
Normal
>40% inspiratory increase
Normal
Ventricular septal shift
Present
Absent
Pericardial thickness >3mm (on transesophageal echocardiography)
Present
Absent
Pericardial effusion
Present
Absent
Plethoric inferior vena cava
Present
Present
Increased ventricular wall thickness
Absent
Present
Pulmonary hypertension
Absent
Present
Cardiac Computerized Tomography
Pericardial thickness
Present
Absent
Calcified pericardium
Present
Absent
Biatrial enlargement
Absent
Present
Cardiac Contour deformation
Present
Absent
Cardiac Magnetic Resonance Imaging
Pericardial thickness
Increased
Normal
Pericardial Inflammation
Increased
Absent
Respirophasic shift
Increased
Absent
Septal bounce
Present
Absent
Wall thickness
Normal
Abnormal
Myocardial delayed enhancement
Absent
Abnormal
Cardiac Catheterization (gold standard)
Equalization of end-diastolic pressure
Present
Present
Low cardiac output
Present
Present
Square root sign
Present
Present
Systolic area index >1.1
Present
Absent
Right ventricular end-diastolic/Right ventricular systolic pressure >0.33
Present
Absent
Respirophasic ventricular pressure changes
Discordant
Concordant
Table 2: Differentiating features of Constriction and Restriction - Clinical, Echocardiographic, Cardiac computerized tomography, Cardiac magnetic resonance imaging and Catheterization. Adapted from Geske et al (2016)12
To confirm the diagnosis of CP, cardiac catheterization is performed to evaluate hemodynamics, specifically diastolic equalization of pressures in all cardiac chambers along with discordant changes in left and right ventricular systolic pressures with respiration prior to undergoing pericardiectomy. However, in our case, ventricular pressure changes were concordant consistent with restrictive physiology. Hence, it revealed that our patient had imaging features of both the constrictive pericarditis and restrictive cardiomyopathy.
Patients with confirmed constrictive pericarditis unresponsive to medical therapy should undergo radical pericardiectomy. However, it is important to be aware that patients with constrictive pericarditis due to radiation heart disease undergoing pericardiectomy have increased mortality compared to the other etiologies.9-10 Unfortunately, mortality in patients with mixed pericardial constriction and restrictive cardiomyopathy is also higher compared to pericardial constriction alone.11 Furthermore, it has been reported that after excluding for patients with radiation exposure, pericardial constriction in patients with a moderate compared to mild or no tricuspid regurgitation is associated with higher mortality after pericardiectomy.10
It was difficult to predict whether patient's symptoms would improve or worsen after pericardiectomy. Anti-inflammatory therapy could have been beneficial had this been transient constrictive pericarditis.7 Tricuspid regurgitation and right ventricular systolic function could worsen postoperatively and further complicate outcomes after pericardiectomy. Conversely, delaying surgical management could worsen overall prognosis and increase mortality. After detailed discussion with the patient, the patient opted for continued medical therapy with close outpatient follow up.
Table 1B: Pressure recordings from cardiac catheterization of right atrium, right ventricle, left atrium and left ventricle showing equalization of pressures.
Video 1B
Video 1B
Video 1B: Cardiac magnetic resonance imaging free breathing cine sequence showing respirophasic septal shift.
Video 1B: Cardiac magnetic resonance imaging free breathing cine sequence showing respirophasic septal shift.
References
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC). Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Hear J 2015;36:2921-64.
Welch TD, Ling LH, Espinosa RE, et al. Echocardiographic diagnosis of constrictive pericarditis: Mayo Clinic criteria. Circ Cardiovasc Imaging 2014;7:526-34.
Talreja DR, Edwards WD, Danielson GK, et al. Constrictive pericarditis in 26 patients with histologically normal pericardial thickness. Circulation 2003;108:1852-57.
Cremer PC, Tariq MU, Karwa A, et al. Quantitative assessment of pericardial delayed hyperenhancement predicts clinical improvement in patients with constrictive pericarditis treated with anti-inflammatory therapy. Circ Cardiovasc Imaging 2015;8:1-7.
Zurick AO, Bolen MA, Kwon DH, et al. Pericardial delayed hyperenhancement with CMR imaging in patients with constrictive pericarditis undergoing surgical pericardiectomy: a case series with histopathological correlation. JACC Cardiovasc Imaging 2011;4:1180-91.
Feng D, Glockner J, Kim K, et al. Cardiac magnetic resonance imaging pericardial late gadolinium enhancement and elevated inflammatory markers can predict the reversibility of constrictive pericarditis after antiinflammatory medical therapy: a pilot study. Circulation 2011;124:1830-37.
Thavendiranathan P, Verhaert D, Walls MC, et al. Simultaneous right and left heart real-time, free-breathing CMR flow quantification identifies constrictive physiology. JACC Cardiovasc Imaging 2012;5:15-24.
Bertog SC, Thambidorai SK, Parakh K, et al. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol 2004;43:1445-52.
Góngora E, Dearani JA, Orszulak TA, Schaff HV, Li Z, Sundt TM III. Tricuspid regurgitation in patients undergoing pericardiectomy for constrictive pericarditis. Ann Thorac Surg 2008;85:163-70.
Yamada H, Tabata T, Jaffer SJ, et al. Clinical features of mixed physiology of constriction and restriction: echocardiographic characteristics and clinical outcome. Eur J Echocardiogr 2007;8:185-94.
Geske JB, Anavekar NS, Nishimura RA, Oh JK, Gersh BJ. Differentiation of constriction and restriction: complex cardiovascular hemodynamics. J Am Coll Cardiol 2016;68:2329-47.