A 71-year-old man presented to our hospital with a one-month history of worsening dyspnea (NYHA 3), lower limb edema, and abdominal distension. A computerized tomography (CT) scan showed the presence of ascites and a cirrhotic appearing liver. Physical exam revealed normal vital signs, elevated jugular venous pulse, a distended abdomen, and 3+ pedal edema. Electrocardiogram and chest x-ray were unremarkable. Inflammatory markers were unremarkable with a normal C-reactive protein of (0.32 mg/dL). Initial echocardiogram findings are shown in Figures 1-3.
Figure 1
Figure 1
Figure 1: Transthoracic parasternal long axis (top) and apical 4-chamber view (bottom). In both images, there is a prominent diastolic septal bounce. In the apical 4-chamber view, there are signs of ventricular interdependence. There is also extra-echoic signs at the apex suggestive of a thickened adherent pericardium or fibro-adhesive material.
Figure 1: Transthoracic parasternal long axis (top) and apical 4-chamber view (bottom). In both images, there is a prominent diastolic septal bounce. In the apical 4-chamber view, there are signs of ventricular interdependence. There is also extra-echoic signs at the apex suggestive of a thickened adherent pericardium or fibro-adhesive material.
Figure 2
Figure 2
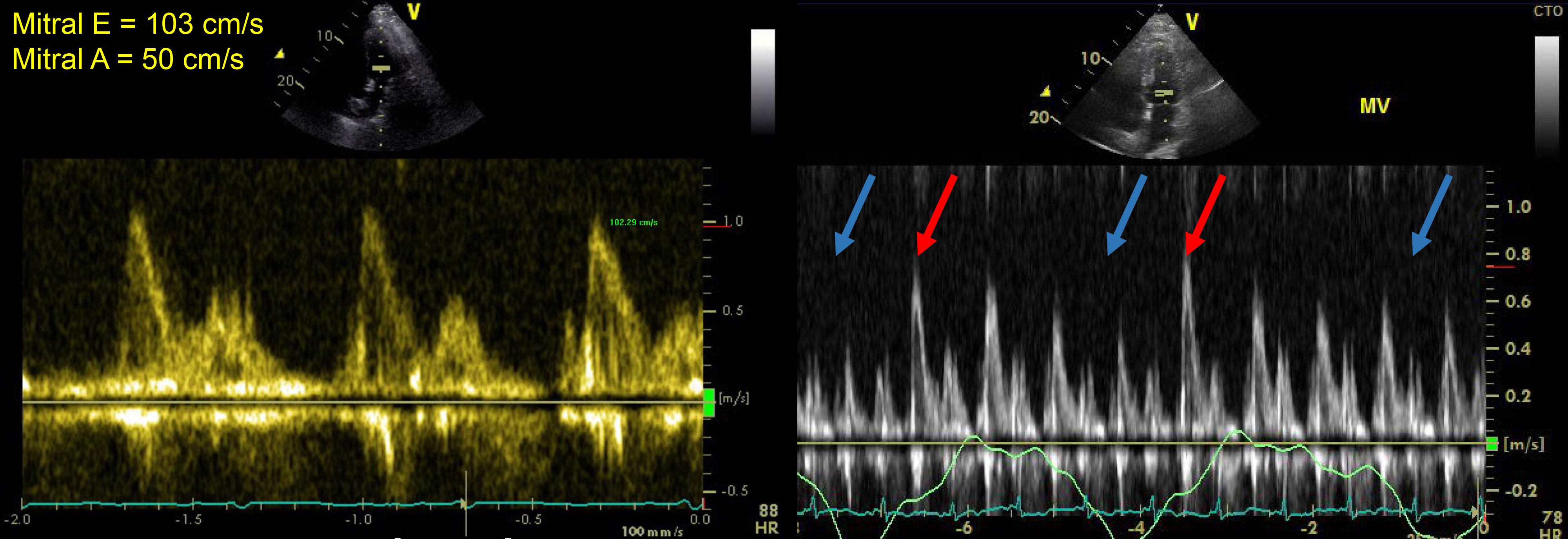
Figure 2: Transthoracic echocardiography mitral valve inflow tracings (left) and with respiration (right). Right image: blue arrows denote expiration, red arrows denote inspiration.
Figure 2: Transthoracic echocardiography mitral valve inflow tracings (left) and with respiration (right). Right image: blue arrows denote expiration, red arrows denote inspiration.
Figure 3
Figure 3
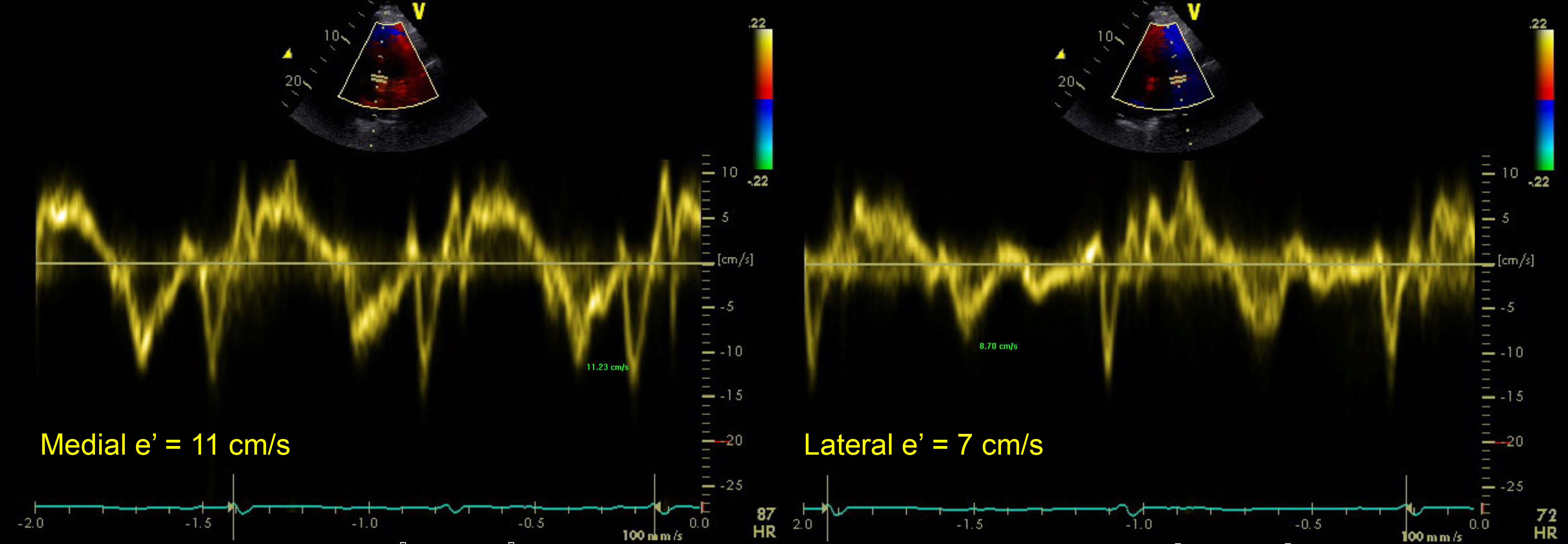
Figure 3: Transthoracic echocardiography Doppler tracings of the medial (left) and lateral (right) annulus.
Figure 3: Transthoracic echocardiography Doppler tracings of the medial (left) and lateral (right) annulus.
Subsequently, the patient underwent a simultaneous left and right cardiac catheterization (Figure 4) and subsequently a cardiovascular magnetic resonance imaging (CMR) (Figure 5).
Figure 4
Figure 4
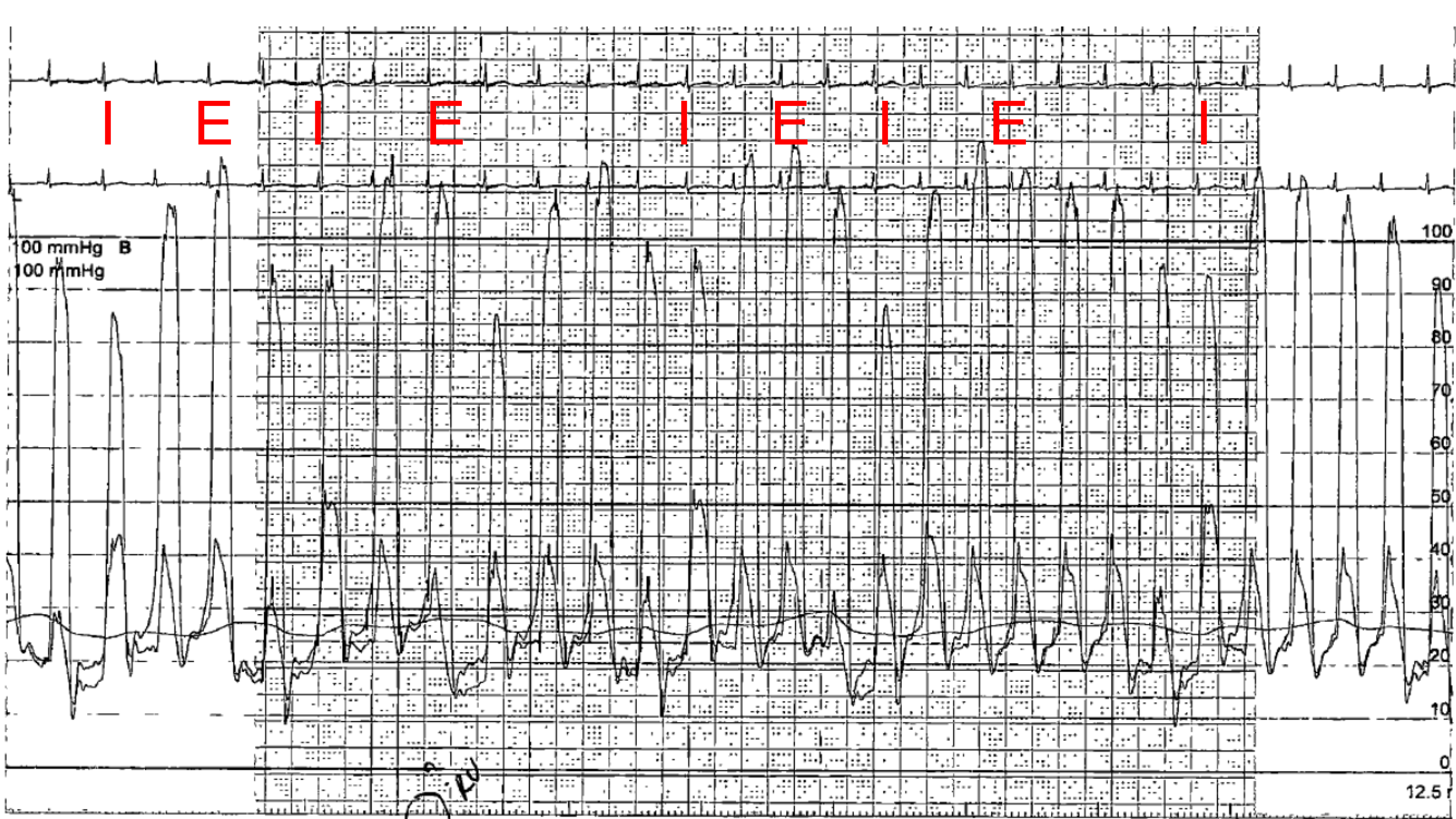
Figure 4: Simultaneous cardiac catheterization tracings of the left and right ventricle. I = Inspiration E = Expiration.
Figure 4: Simultaneous cardiac catheterization tracings of the left and right ventricle. I = Inspiration E = Expiration.
Figure 5
Figure 5
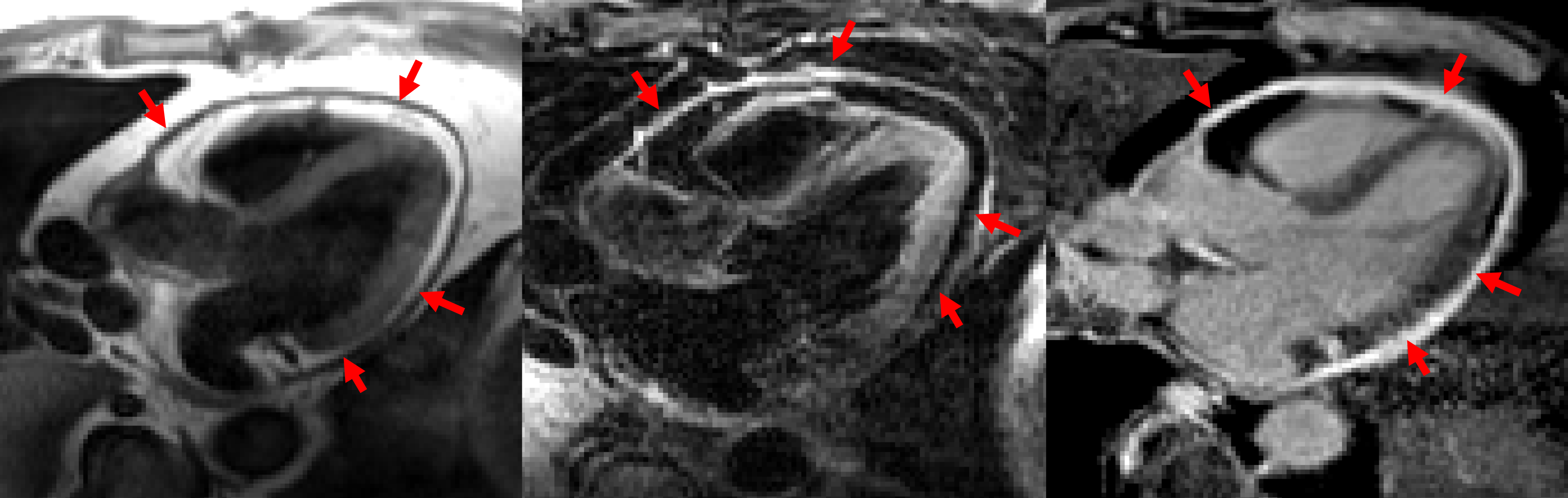
Figure 5: CMR images with the T1 weighted imaging (left), T2 weighted with fat saturation (middle), and late gadolinium enhancement-fat saturation (right) sequences. T1 weighted image (left): Globally thickened pericardium of 5 mm.
T2 weighted image with fat saturation (middle): Global hyperintense pericardium suggestive of edema.
Late gadolinium enhancement-fat saturation (right): Global hyperintense pericardium suggestive of active inflammation.
Figure 5: CMR images with the T1 weighted imaging (left), T2 weighted with fat saturation (middle), and late gadolinium enhancement-fat saturation (right) sequences. T1 weighted image (left): Globally thickened pericardium of 5 mm.
T2 weighted image with fat saturation (middle): Global hyperintense pericardium suggestive of edema.
Late gadolinium enhancement-fat saturation (right): Global hyperintense pericardium suggestive of active inflammation.
What is the clinical diagnosis and best next step in management?
Show Answer
The correct answer is: D. Constrictive pericarditis, trial of anti-inflammatory therapy and corticosteroids
In this case, the echocardiography demonstrated ventricular interdependence with presence of a septal bounce (Figure 1), restrictive mitral filling pattern (Figure 2), mitral respirophaic changes in Doppler velocity (Figure 2), as well as annulus reversus (Figure 3) – a tissue Doppler finding where the medial tissue Doppler is normal or higher than the lateral tissue Doppler. Cardiac catheterization (Figure 4) showed many features of constriction, including a rapid filling wave, equalization of LV and RV end diastolic pressures, and ventricular discordance with respiration. The CMR (Figure 5) demonstrated a circumferentially thickened pericardium (5 mm) with avid inflammation and edema, as depicted on the T2 and late gadolinium enhancement sequences.
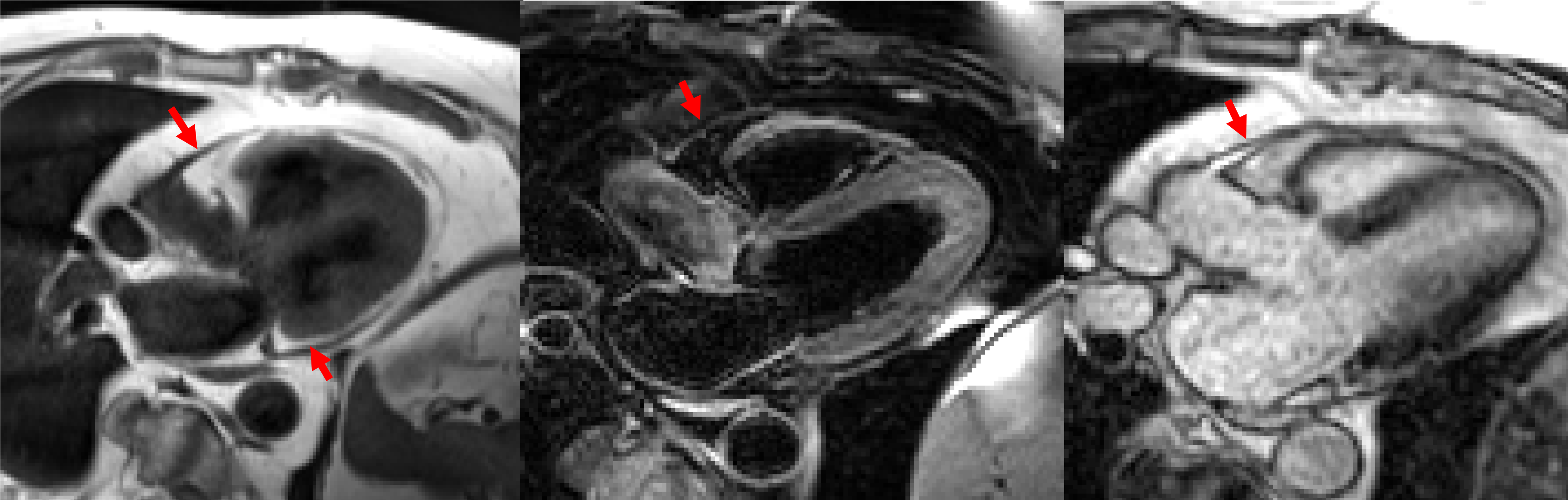
Based on the presence of the CMR findings, a diagnosis of transient constrictive pericarditis was made, and the patient was treated with a prolonged course of anti-inflammatory therapy. A CMR follow-up at one year showed marked improvement of pericardial thickness and inflammation (Figure 6).
Figure 6
Figure 6
Figure 6: CMR images at 1 year follow-up the T1 weighted imaging (left), T2 weighted with fat saturation (middle), and late gadolinium enhancement (right) images acquired. T1 weighted image (left): Focal areas of thickened pericardium.
T2 weighted image with fat saturation (middle): Small area of pericardial edema present.
Late gadolinium enhancement-fat saturation (right): Small area of inflammation present.
Figure 6: CMR images at 1 year follow-up the T1 weighted imaging (left), T2 weighted with fat saturation (middle), and late gadolinium enhancement (right) images acquired. T1 weighted image (left): Focal areas of thickened pericardium.
T2 weighted image with fat saturation (middle): Small area of pericardial edema present.
Late gadolinium enhancement-fat saturation (right): Small area of inflammation present.
Transient constrictive pericarditis was first described in 1987 with 16 patients who presented with physical exam and echocardiographic findings of constriction but which, within a few months, spontaneously resolved on later echocardiographic and cardiac catheterization studies.1 In transient constriction, the histology of the pericardium reveals inflammation with vascularization granulation tissue and fibrin deposition, unlike the changes seen in chronic constrictive pericarditis with the abundance of fibroblasts and collagen.2
Following acute pericarditis, transient constrictive physiology occurs in up to 15% of patients, as detected using echocardiography, and represents a much larger than the 2% of patients who progress to chronic constrictive pericarditis.3 Conversely, transient constrictive pericarditis occurs in 17% of patients that present with signs and symptoms of constriction physiology.4 Although most commonly from idiopathic or viral induced pericarditis, transient constriction can occur with almost all other etiologies of pericarditis, with the exception of radiation.4
CMR is well suited to assess pericardial thickness and inflammation. Using T1 spin-echo sequences the thickness of the pericardium can be measured, with a value of >4 mm as being abnormal.5 T2 spin-echo sequences can evaluate pericardial edema while late gadolinium enhancement sequences can assess for pericardial inflammation.6 Cardiac computerized tomography (CT) can show a thickened pericardium and importantly the lack of pericardial calcification.7 Inflammatory markers are also commonly elevated, but can be negative in 25% of individuals.8
After detection of active pericardial inflammation, treatment with NSAIDs/aspirin, colchicine, and corticosteroids should be initiated.7 Although initially avoided in acute pericarditis, corticosteriods, in combination with other anti-inflammatory therapy, may be more suitable in cases with intense pericardial inflammation.9 Guidelines recommend 2-3 months of anti-inflammatory therapy, although tailoring therapy with repeated CMRs to evaluate for ongoing inflammation may be beneficial.9
References
Sagrista-Sauleda J, Permanyer-Miralda G, Candell-Riera J, Angel J, Soler-Soler J. Transient cardiac constriction: an unrecognized pattern of evolution in effusive acute idiopathic pericarditis. J Am J Cardiol 1987;59:961-6.
Taylor AM, Dymarkowski S, Verbeken EK, Bogaert J. Detection of pericardial inflammation with late-enhancement cardiac magnetic resonance imaging: initial results. Eur Radiol 2006;16:569-74.
Imazio M, Brucato A, Maestroni S et al. Risk of constrictive pericarditis after acute pericarditis. Circulation 2011;124:1270-5.
Haley JH, Tajik AJ, Danielson GK, Schaff HV, Mulvagh SL, Oh JK. Transient constrictive pericarditis: causes and natural history. J Am J Cardiol 2004;43:271-5.
Bogaert J, Francone M. Cardiovascular magnetic resonance in pericardial diseases. J Cardiovasc Magn Reson 2009;11:14.
Rajiah P. Cardiac MRI: Part 2, pericardial diseases. AJR Am J Roentgenol 2011;197:W621-34.
Adler Y, Charron P, Imazio M et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Euro Heart J 2015;36:2921-64.
Imazio M, Brucato A, Maestroni S et al. Prevalence of C-reactive protein elevation and time course of normalization in acute pericarditis: implications for the diagnosis, therapy, and prognosis of pericarditis. Circulation 2011;123:1092-7.
Gentry J, Klein AL, Jellis CL. Transient constrictive pericarditis: current diagnostic and therapeutic strategies. Curr Cardiol Rep 2016;18:41.