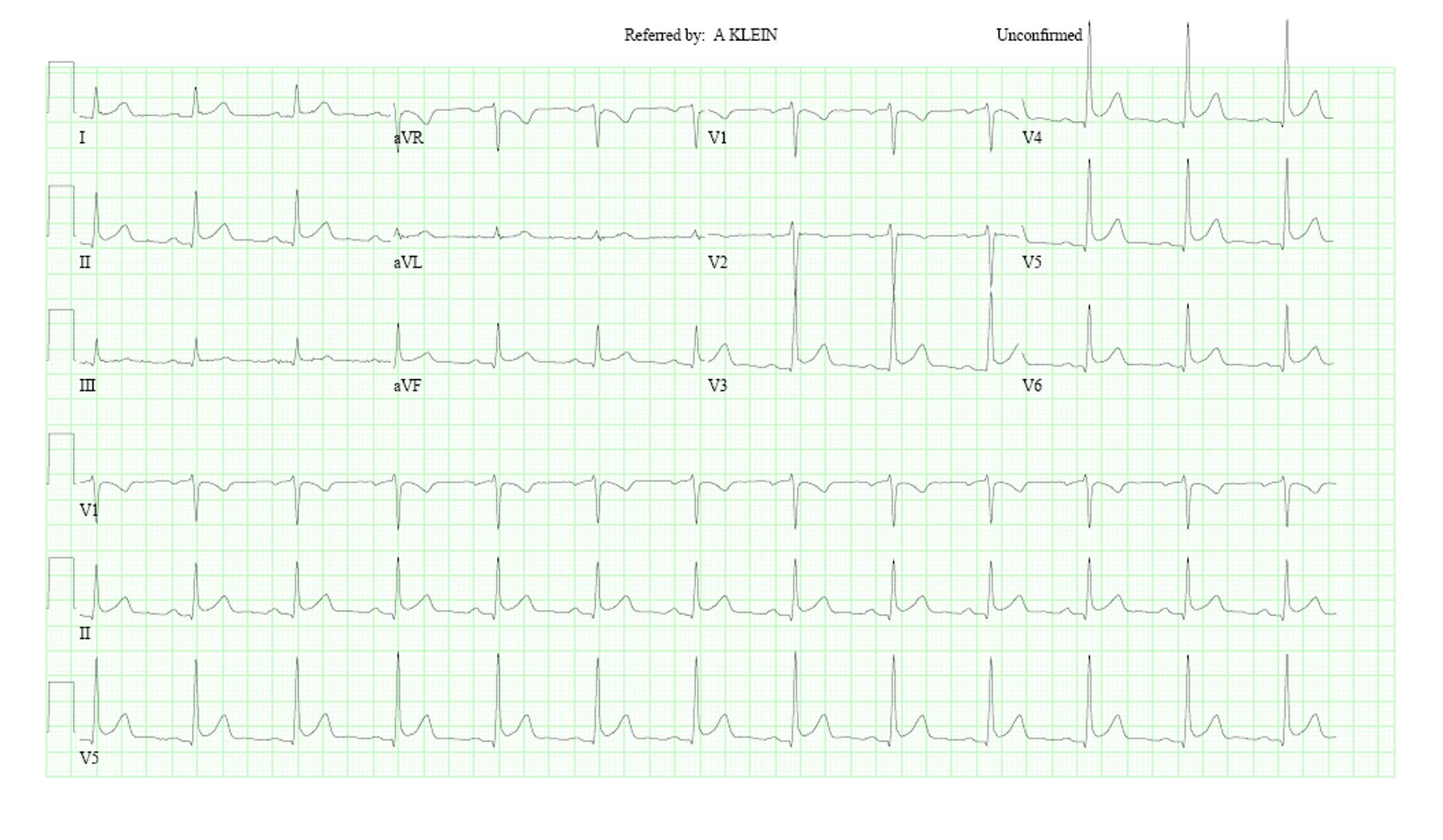
A 33 year-old gentleman presented to the pericardial diseases center with chest pain. Eight years prior to presentation, he was hospitalized with pneumonia and chest pain. An electrocardiogram (ECG) was performed at that time and reportedly showed diffuse ST segment elevations. He was diagnosed with pericarditis and started on colchicine and nonsteroidal anti-inflammatory drugs (NSAIDs). Over the years, he also received many courses of steroids. None of these treatments provided relief of chest pain which was described as left-sided, axillary in location, and worse with raising the left arm above his head. The pain is associated with attendant left arm tingling and numbness extending to the hand. In contrast, there is no relationship to exertion or other changes in body positions. Laboratory testing revealed normal erythrocyte sedimentation rate and ultrasensitive C-reactive protein (CRP). Transthoracic echocardiogram (TTE) was normal, without any pericardial effusion or thickening. The ECG obtained in clinic is seen below.
Figure 1
Figure 1
This patient's symptoms and diagnostic findings are most suggestive of which of the following diagnoses?
Show Answer
The correct answer is: E. Two of the above
This patient has musculoskeletal pain in the setting of Benign Early Repolarization.
To diagnose pericarditis, one needs two of the following four findings: 1) typical chest pain (worse with inspiration and supine position), 2) characteristic ECG findings including ST segment elevation and PR depression, 3) a pericardial friction rub, and 4) a non-trivial pericardial effusion.1
The ECG findings in the acute pericarditis have four stage evolution. First stage occurs within hours to days. It involves diffuse ST elevation (except in aVR and often V1) along with PR depression. Second stage occurs after one week and involves return to baseline of acute ST and PR deviations along with T wave flattening. Third stage involves ST segment becoming isoelectric followed by diffuse T wave inversion. Fourth stage involves total normalization ECG or chronic sustained T wave inversions.2
Our patient's ECG demonstrated concave ST elevations in the inferior limb leads and late precordial leads which could suggest pericarditis, but there was terminal QRS slurring,3 high T wave amplitude and the ST:T amplitude ratio was also less than 25%.4 Also, the PR axis was isoelectric and heart rate was normal. Lastly, vector cardiography was normal.5 By this we mean ST and T vectors are parallel and oriented with the QRS axis. These findings suggest the electrocardiographic diagnosis of 'Benign Early Repolarization' rather than pericarditis. Moreover, the description of chest pain is most consistent with musculoskeletal origin, possibly owing to a thoracic outlet syndrome given the predictable worsening with raising the arm over the head.
This patient possessed none of the other findings on our assessment. We cannot say with confidence that these diagnostic findings were not present eight years ago, though the lack of any such findings at this time and presence of normal inflammatory markers were rather convincing. Colchicine and NSAIDs were discontinued and the patient was tapered off of his steroid regimen.
References
Cremer PC, Kumar A, Kontzias A, et al. Complicated pericarditis: understanding risk Factors and pathophysiology to inform imaging and treatment. J Am Coll Cardiol 2016;68:2311-28.
Spodick DH. The Pericardium: A Comprehensive Textbook. Taylor & Francis Group;1996.
Macfarlane PW, Antzelevitch C, Haissaguerre M, et al. The early repolarization pattern: a consensus paper. J Am Coll Cardiol 2015;65:470-77.
Ginzton LE, Laks MM. The differential diagnosis of acute pericarditis from the normal variant: new electrocardiographic criteria. Circulation 1982;65:1004-9.
Hurst, JW. Ventricular Electrocardiography. New York: Gower Medical Publishing;1991: Chapter 10.