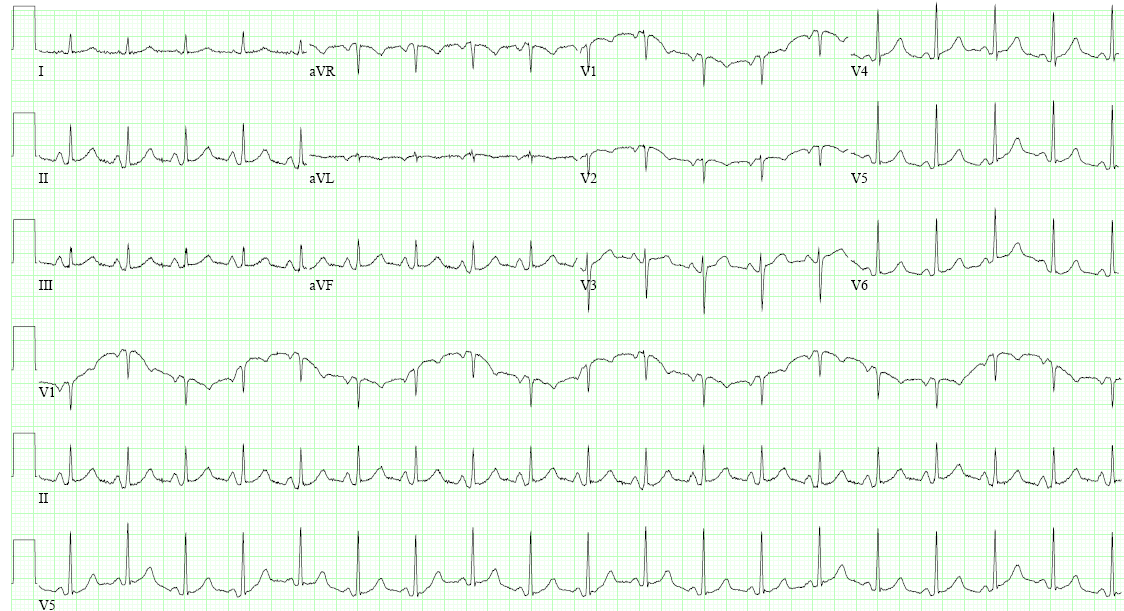
A 54-year-old woman with a past medical history significant for tobacco abuse and hypertension presents with worsening chest discomfort, dyspnea, and weight loss. On admission temperature is 35.6°C, blood pressure 110/65, heart rate 81, respiratory rate, 26, oxygen saturation 95% on 2L. ECG shown in Figure 1. Echocardiogram shown in Figure 2. After admission, patient presents with progressive hypotension and tachycardia. She subsequently underwent pericardiocentesis, improving her hemodynamics. Subsequent pericardial cytology shown metastatic large cell lung cancer, shown in Figure 3.
Figure 1
Figure 1
Figure 2
Figure 2
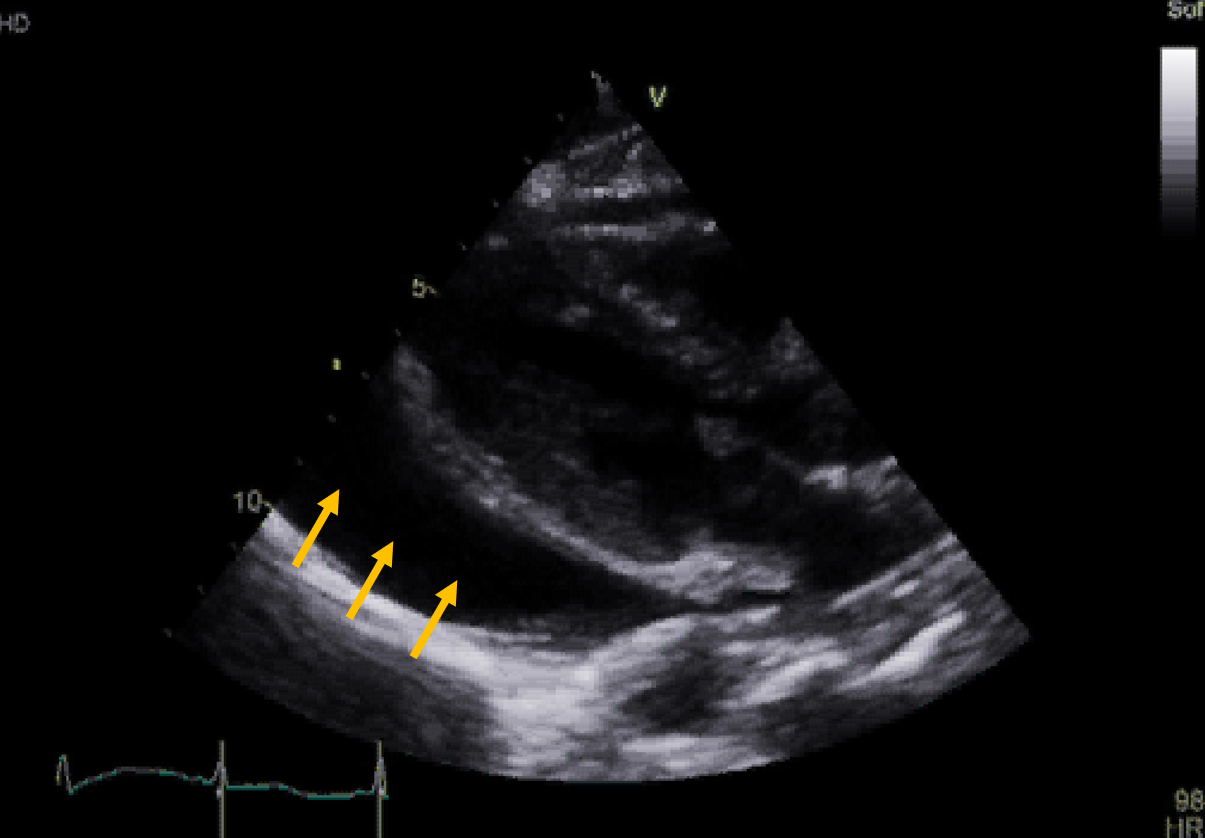
Figure 2: Transthoracic echocardiogram with parasternal long axis view. Arrows point to pericardial effusion
Figure 2: Transthoracic echocardiogram with parasternal long axis view. Arrows point to pericardial effusion
Figure 3
Figure 3
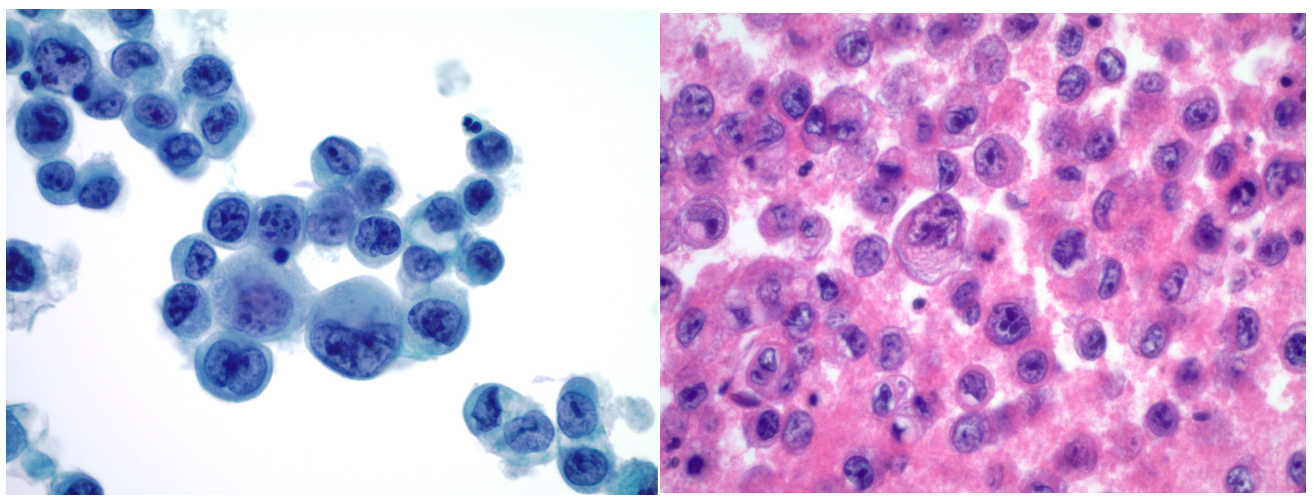
Figure 3: Pericardial fluid cytology showing metastatic large cell carcinoma.
Figure 3: Pericardial fluid cytology showing metastatic large cell carcinoma.
Which of the following pericardial fluid chemistry would you most expect in this patient?
Show Answer
The correct answer is: A. Serum LDH 200 U/L, Fluid LDH 166, Serum protein 7.1 g/dL, Fluid protein 6.1 g/dL
This patient has a malignant pericardial effusion from metastatic large cell lung cancer, as diagnosed by pericardial cytology. Pericardial fluid from malignancy is an exudative process, meaning solute within the pericardium causes water to osmose out of capillary beds into the pericardial space. In this example, malignant cells and subsequent inflammation in the pericardial space cause increased capillary permeability and subsequent fluid flow from capillaries to the pericardial space. In a transudate, fluid enters the pericardial space due to increased capillary hydrostatic pressure or low plasma oncotic pressure. While exudate and transudate are defined mechanistically, Light's criteria (below) has traditionally been used to characterize the chemistry profile of transudate versus exudate. In pericardial effusion, Light's criteria has approximately 90-95% sensitivity for differentiating transudate versus exudate. However, in pericardial effusion, specificity is low between 30-40%. Common causes of pericardial exudate include: malignancy, infection, collagen-vascular disease, post pericardiotomy, acute idiopathic pericarditis. Common transudative etiologies include: uremia, radiation, decompensated heart failure, and hypothyroidism. In the above example, (A) is the only answer that meets Light's criteria for exudate. The others are all transudative chemistry profiles.
Light's Criteria: Must meet one of the following:
Pleural fluid protein/serum protein > 0.5
Pleural fluid LDH/serum LDH > 0.6
Pleural fluid LDH > 2/3 lab upper limit of normal
References
Meyers DG, Meyers RE, Prendergast TW. The usefulness of diagnostic tests on pericardial fluid. Chest 1997;111:1213-21.
Light RW, Macgregor MI, Luchsinger PC, Ball WC Jr. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med 1972;77:507-13.
Corey GR, Campbell PT, Van Trigt P, et al. Etiology of large pericardial effusions. Am J Med 1993;95:209-13.
Sagristà-Sauleda J, Mercé J, Permanyer-Miralda G, Soler-Soler J. Clinical clues to the causes of large pericardial effusions. Am J Med 2000;109:95-101.