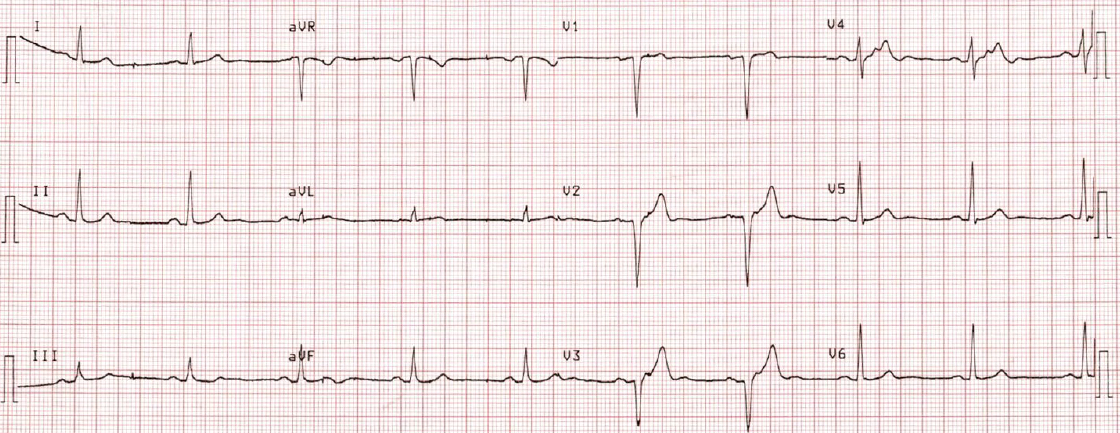
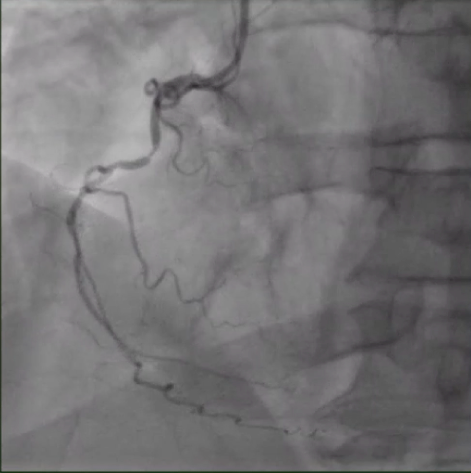
A 60-year old male is seen in clinic to discuss returning to competitive distance running. Three months prior, he suffered ventricular fibrillation cardiac arrest while training for a marathon. After resuscitation in the field, emergent coronary angiography revealed a culprit 95% proximal left anterior descending artery lesion, for which he received a drug eluting stent. Angiography also revealed a 60-70% mid right coronary artery (RCA) stenosis (FFR 0.82), which was not revascularized. In the interim, he successfully completed cardiac rehabilitation with a graded exercise program. Without consulting with a physician, he resumed running 3-4 miles several days per week without angina, dyspnea, dizziness or syncope. His medications include atorvastatin, aspirin, prasugrel, and ramipril. Resting ECG is shown (Figure 1). Angiography of the RCA lesion is shown (Figure 2). Echocardiography revealed a normal left ventricular ejection fraction (LVEF) of 60%, without segmental wall motion abnormalities or valvular pathology. He would like to discuss resuming training for a marathon.
Figure 1
Figure 1
Figure 2
Figure 2
In addition to optimal medical therapy, which of the following is the most appropriate next step in management?
Show Answer
The correct answer is: C. Maximal exercise stress test
Current American College of Cardiology (ACC) and European Association of Preventive Cardiology (EAPC) recommendations suggest shared decision making for athletes returning to play with coronary artery disease.1,2 Despite the absence of symptoms, this patient is at increased risk of exercise-induced adverse cardiac events due to his 60-70 % RCA disease. The 2015 ACC Eligibility and Disqualification Recommendations suggest it is reasonable for asymptomatic patients with known coronary artery disease (CAD) to participate in all competitive activities if their resting left ventricular ejection fraction is >50% and they have no inducible ischemia or electrical instability with maximal stress testing (Class IIb; LOE: C).2 Given the patient strongly desires to return to play, it is reasonable to discuss completing a monitored exercise program, such as cardiac rehab, and subsequently a maximal exercise stress test prior to returning to competitive marathon running.
Recommending restriction from competitive athletics could also be considered. In contrast to the 2015 ACC recommendations, the 2019 EAPC recommendations for athletic participation in patients with CAD recommend restriction from high intensity athletic activity for high risk patients defined as having any of the following: Presence of at least one coronary stenosis of a major coronary artery (>70%) or left main stem (>50%), LVEF <50%, ventricular tachyarrhythmias at any time (including NSVT, PMVT, frequent PVCs), exercise induced ischemia or new left bundle branch block, dyspnea at low exercise intensity (angina equivalent), dizziness or syncope on exertion, or high degree of myocardial scarring on cardiac magnetic resonance (CMR) imaging (Class IIa, LOE: C).1 While this patient did have a dangerous ventricular tachyarrhythmia causing his initial event, the culprit LAD lesion was revascularized and he has no evidence of scar with a normal LVEF and no regional wall motion abnormalities. In an effort to promote shared decision making, we suggest performing a maximal exercise stress test for further risk stratification as the best next step for this patient. Both ACC and EAPC recommendations suggest waiting at least 3 months from acute myocardial infarction or PCI to return to play (Class IIb; LOE C).1,2 Other data suggest a return to competitive sports after up to two years of aggressive lipid lowering therapy in order to allow for optimal myocardial healing and atherosclerotic plaque stabilization.2,4
Percutaneous coronary intervention of the borderline RCA lesion would be reasonable in an asymptomatic patient with CAD if maximal exercise stress testing revealed ischemia in its territory or if anti-ischemic medical therapy was limiting performance. EAPC recommendations suggest a more aggressive revascularization strategy for athlete-patients who wish to participate in competitive sports, including asymptomatic patients with inducible ischemia (N.B.: expert consensus),1,3 while ACC recommendations suggest restricting patients with atherosclerotic coronary artery disease (ASCAD) and inducible ischemia to low dynamic and static demand activity (Class IIb; LOE C).2
Cardiac MRI would be appropriate if prior testing for risk stratification, including stress testing, was not conclusive.
Prior to starting an aggressive training program, the patient developed progressive angina. He ultimately underwent revascularization of the RCA with a drug eluting stent, resolving his symptoms. Afterwards, he gradually increased his exercise activity in and outside of cardiac rehabilitation. He underwent a maximal symptom limited stress test which was negative for ischemia or ventricular arrhythmias, and with shared decision making greater than 3 months after the stent, subsequently participated noncompetitively in a 10-mile road race.
References
Borjesson M, Dellborg M, Niebauer J, et al. Recommendations for participation in leisure time or competitive sports in athletes-patients with coronary artery disease: a position statement from the Sports Cardiology Section of the European Association of Preventive Cardiology (EAPC), Eur Heart J 2019;40:13-18.
Thompson PD, Myerburg RJ, Levine BD, Udelson JE, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 8: coronary artery disease: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015;66:2406–11.
Cook CM, Ahmad Y, Howard JP, et al. Impact of percutaneous revascularization on exercise hemodynamics in patients with stable coronary disease. J Am Coll Cardiol 2018;72:970–83.
Zhao XQ, Dong L, Hatsukami T, et al. MR imaging of carotid plaque composition during lipid-lowering therapy a prospective assessment of effect and time course. JACC Cardiovasc Imaging 2011;4:977–86.