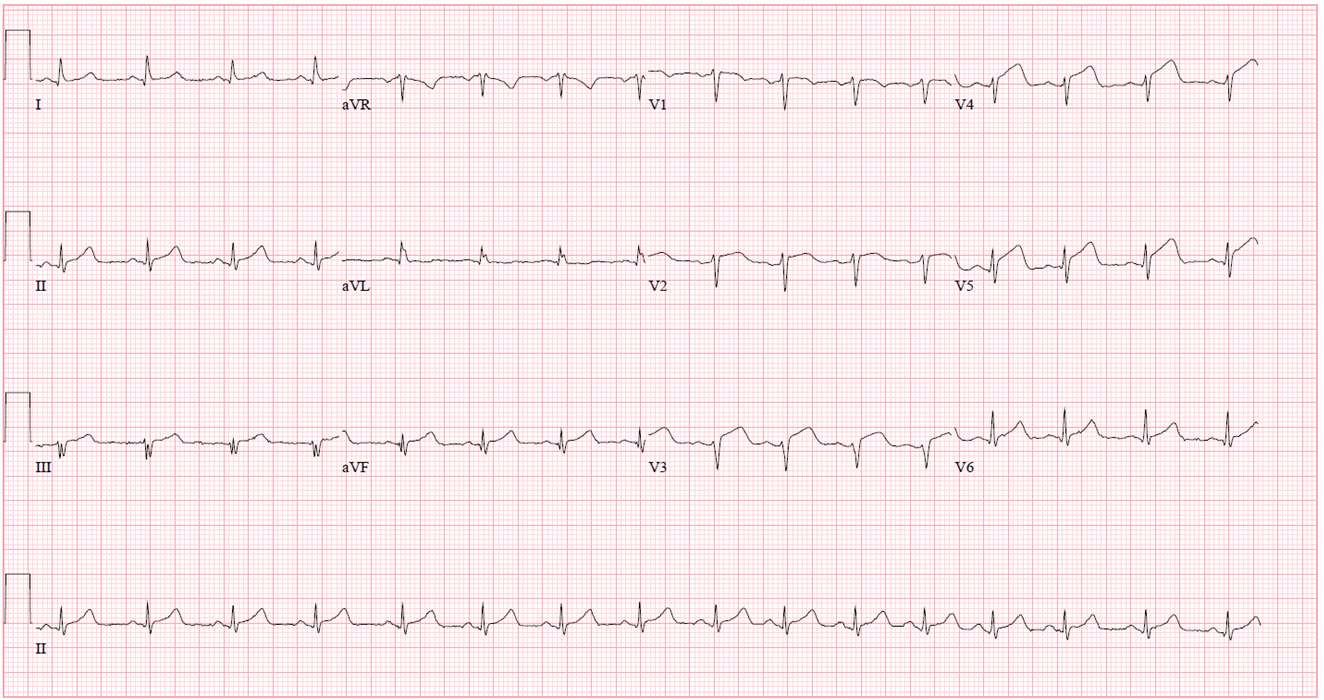
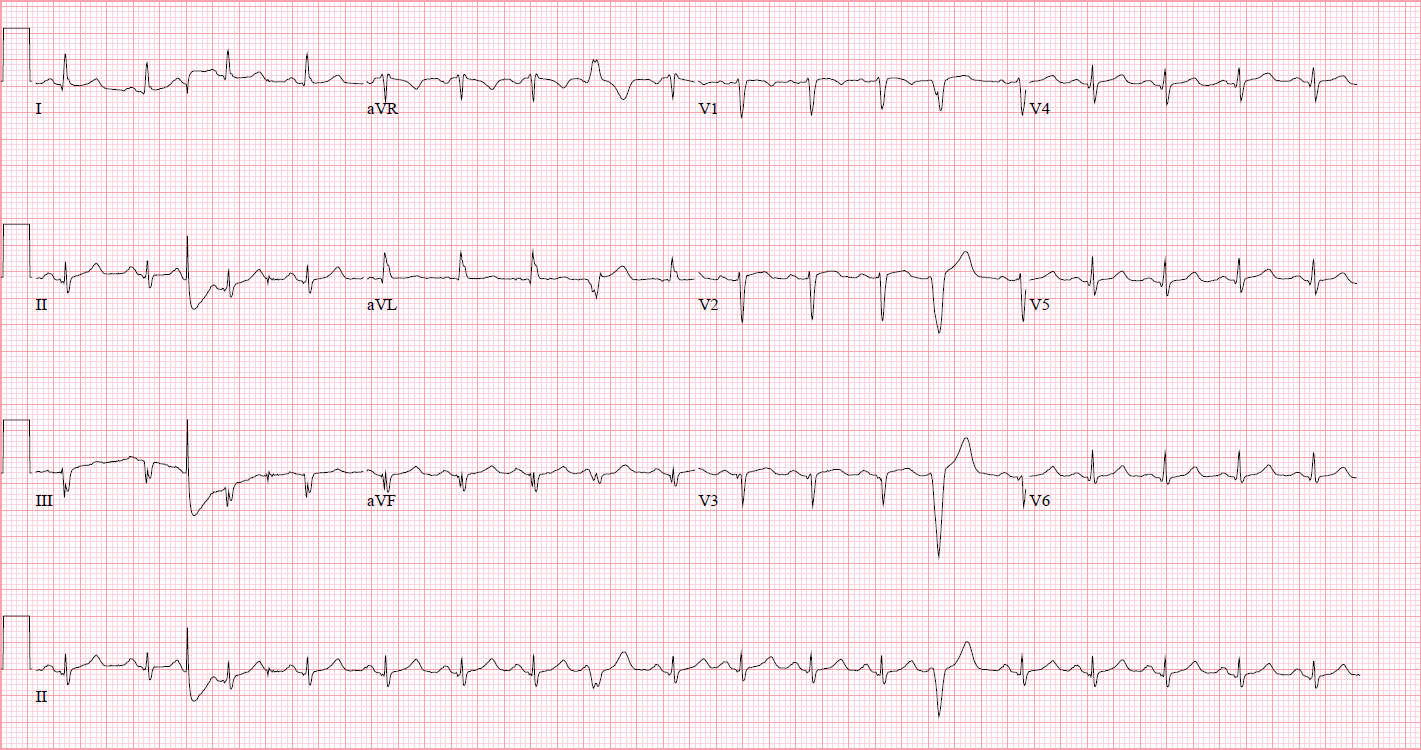
A 36-year-old woman presented to the emergency room with severe chest pressure for 25 minutes while driving. The chest pain was sub-sternal in nature, radiating to right chest. She denies any associated dizziness or palpitations or syncope. She denies any drug abuse. Her past medical history is significant for obesity, migraine, gastroesophageal reflux disease and fibromyalgia. Family history is significant for a deceased sister from cardiopulmonary arrest 5 months after bariatric surgery. Physical examination was grossly normal. Electrocardiogram is shown in Figure 1. Emergent coronary angiogram was performed (Figure 2, Videos 1 and 2).
Figure 1: Baseline Electrocardiogram
Figure 1
Figure 2
Figure 2
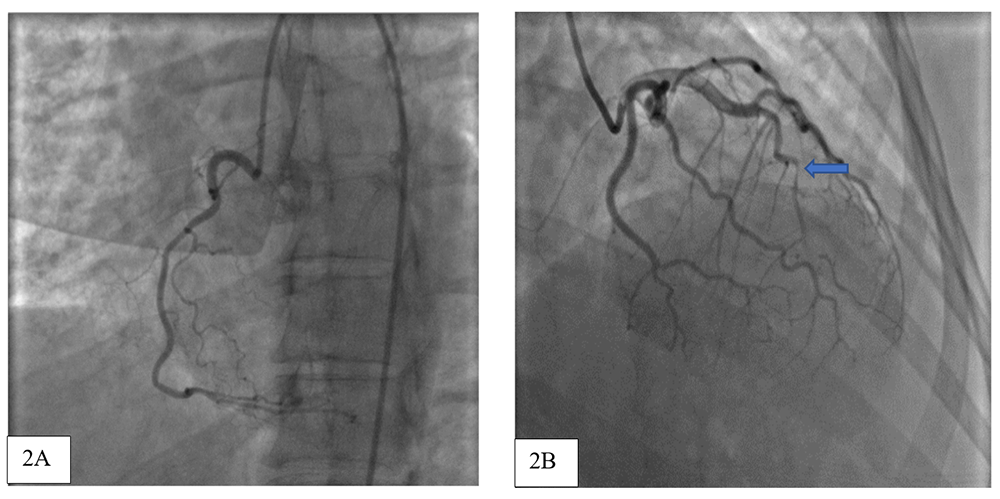
Figure 2: Normal right coronary system (Figure 2A), and tortuous left anterior descending artery (LAD), with spontaneous dissection of mid LAD after first diagonal and second septal (arrow, Figure 2B) with total occlusion of distal LAD segment.
Figure 2: Normal right coronary system (Figure 2A), and tortuous left anterior descending artery (LAD), with spontaneous dissection of mid LAD after first diagonal and second septal (arrow, Figure 2B) with total occlusion of distal LAD segment.
Video 1
Video 1
Video 2
Video 2
What is the etiology behind acute myocardial infarction?
Show Answer
The correct answer is: D. Spontaneous coronary artery dissection.
Figure 2 (and Video 1) demonstrate a normal right coronary system, and a tortuous left anterior descending artery (LAD), with spontaneous type dissection of mid LAD after first diagonal and second septal with total occlusion of distal LAD segment. Left ventriculogram demonstrated anteroapical dyskinesis (Video 2). Patient subsequently underwent balloon angioplasty and drug eluting stent placement in mid-distal LAD (2.5x38 mm and 2.75x16 mm drug eluting stents) with restoration of TIMI III flow (Video 3) and resolution of ST segment elevations on electrocardiogram (Figure 3).
Video 3
Video 3
Figure 3
Figure 3
Figure 3: 12 lead electrocardiogram post cardiac catherization demonstrating resolution of ST-segment elevation
Figure 3: 12 lead electrocardiogram post cardiac catherization demonstrating resolution of ST-segment elevation
Spontaneous coronary artery dissection (SCAD) is defined as spontaneous separation of coronary artery wall in absence of any trauma or surgical instrumentation or catheter manipulation. This is a rare cause of myocardial infarction and sudden cardiac death. Although the true prevalence of SCAD is unknown, there is increased female predominance with mixed results.1,2 There should be high suspicion for SCAD in young women presenting with myocardial infarction (MI), with contemporary data suggesting a SCAD prevalence of 22% to 43% in this patient population.2-4 Another clue to the presence of SCAD in our case is the excessive tortuosity of LAD. SCAD can be angiographically classified into three different subtypes – type 1 is characterized by arterial wall contrast staining with multiple radiolucent lumen; type 2 is characterized by diffuse stenosis of varying severity and length; and type 3 is characterized by focal or tubular stenosis and requires intracoronary imaging to confirm the presence of an intramural hematoma.5 Although a significant proportion of SCAD cases demonstrate healing during follow-up angiography, revascularization (either bypass surgery or percutaneous coronary intervention) should be considered in a setting of ongoing ischemia (like ours), hemodynamic instability, large myocardial infarction or cardiac arrest.5 Our case demonstrates successful percutaneous coronary intervention of SCAD involving mid-distal LAD in the setting of anterior MI and ongoing ischemia.
References
Garg J, Krishnamoorthy P, Palaniswamy C, Pandey A, Ahmad H. Predictors of in-hospital mortality in coronary artery dissection: findings from the National Inpatient Sample 2009-2010. Cardiol J 2015;22:135-40.
Rashid HN, Wong DT, Wijesekera H, et al. Incidence and characterisation of spontaneous coronary artery dissection as a cause of acute coronary syndrome--a single-centre Australian experience. Int J Cardiol 2016;202:336-8.
Elkayam U, Jalnapurkar S, Barakkat MN, et al. Pregnancy-associated acute myocardial infarction: a review of contemporary experience in 150 cases between 2006 and 2011. Circulation 2014;129:1695-702.
Sharma S, Kaadan MI, Duran JM, et al. Risk factors, imaging findings, and sex differences in spontaneous coronary artery dissection. Am J Cardiol 2019;123:1783-87.
Saw J, Mancini GBJ, Humphries KH. Contemporary review on spontaneous coronary artery dissection. J Am Coll Cardiol 2016;68:297-312.