The patient is a 66-year-old male with a history of chronic obstructive pulmonary disease, type II diabetes mellitus, hyperlipidemia, tobacco use and known coronary artery disease, s/p PCI 4 years ago. He presents with cough, exertional chest tightness and right arm pain. He is found to have stage IIIB non-small cell lung cancer. He is undergoing evaluation and staging for chemotherapy. The following ECG is performed:
The correct answer is: E. Both A and D.
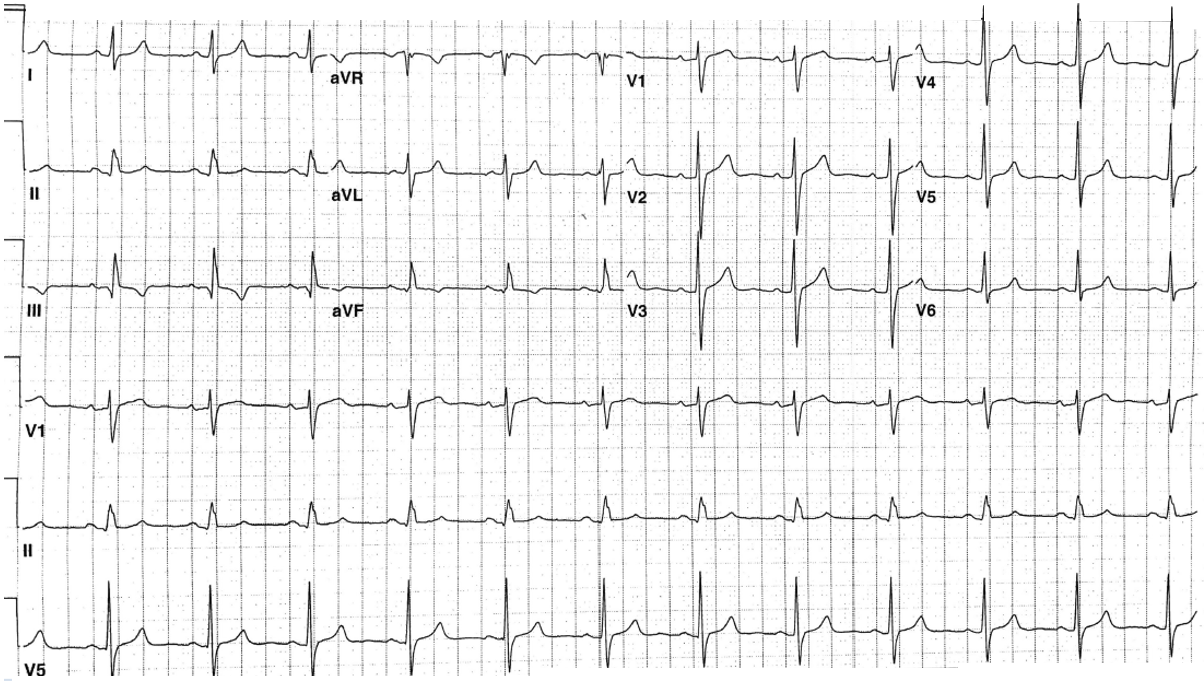
The ECG shows sinus rhythm with a QRS axis of approximately +80 degree. The QRS is minimally wide at 108 milliseconds. Q waves are present in lead II, III, aVF although the Q wave in aVF is borderline wide around 40 milliseconds. This is reflective of the previous inferior infarct, which was noted on echocardiogram with inferior wall akinesis. A stress perfusion study was done, which showed a large inferior infarction defect with minimal reversibility. The inferior infarct of undetermined age because of the T wave negativity in lead II and aVF is additionally manifest by the inferior infarction block with wide initial and terminal forces in aVF (also noted readily in aVR).
References
- Baker JM, Donovan TF, Bakos AC. Alterations in the form of the ventricular complex produced by local intraventricular block complicating myocardial infarction. Bull Georgetown Univ Med Cent 1949;3:137-46.