A 74-year-old woman presented with worsening exertional dyspnea over the preceding 2 months in the setting of severe calcific aortic stenosis. She had multiple comorbidities including severe chronic obstructive pulmonary disease, history of nephrectomy and ileocolectomy for asynchronous tumors, pulmonary embolism, and rheumatoid arthritis on chronic immunosuppression. After multidisciplinary discussions, she was found to be at high surgical risk and planned for transcatheter aortic valve replacement.
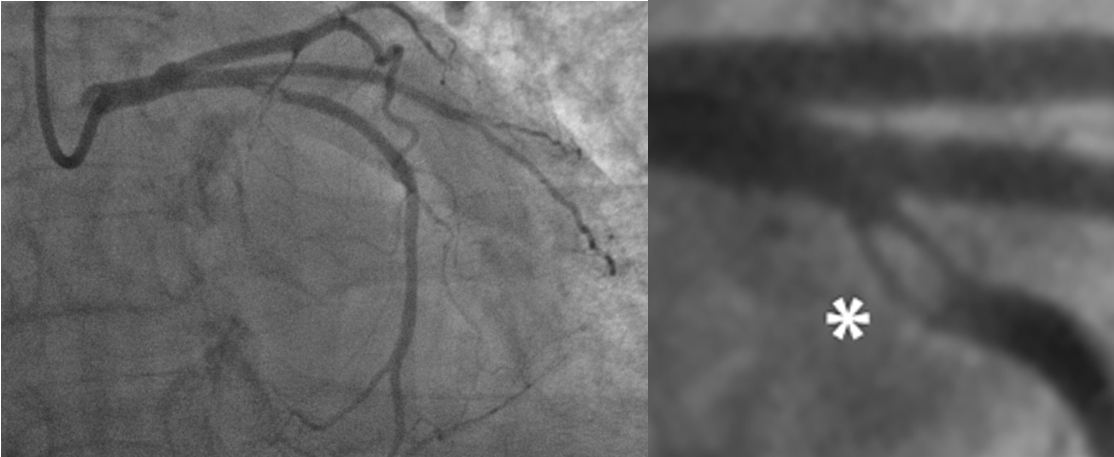
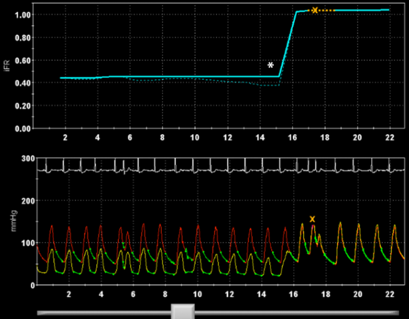
Pre-procedural coronary angiography showed unobstructed coronaries but a focal calcific lesion in the left circumflex artery (LCx) with a dual residual lumen (Figure 1). In view of the unusual angiographic findings, the lesion was evaluated further by optical coherence tomography (OCT) imaging and coronary physiologic assessment. The instantaneous wave-free ratio (iFR) was severely depressed at 0.44 in the distal LCx, with an abrupt gradient at the level of the abnormality (Figure 2).
Figure 1
Figure 1
Figure 2
Figure 2
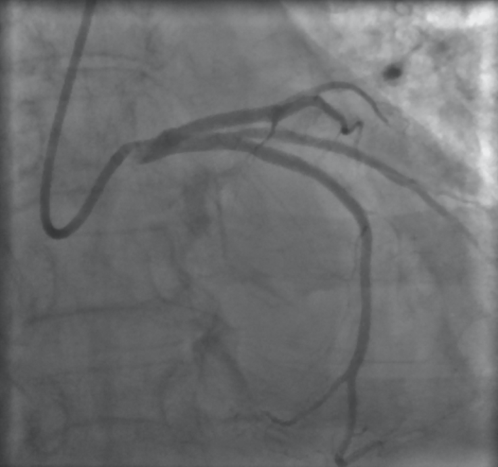
Given the severe, large-territory ischemia, the decision was made to proceed with percutaneous coronary intervention (PCI). The lesion was pre-dilated with a 2.5 mm balloon, and a 3.0 x 15 mm drug-eluting stent was placed, covering the ostium of the obtuse marginal (OM) branch. The stent was post-dilated using a 3.0 mm non-compliant balloon at high pressures (20 atm) with good angiographic result in the main vessel but moderate 40% stenosis of the OM ostium (Figure 3).
Figure 3
Figure 3
What is the next best step in this patient's treatment?
Show Answer
The correct answer is: C. Repeat physiologic assessment of LCx post-PCI.
Physiologic assessment of jailed side branches (answer B) is feasible if the jailed side branch may cause ischemia. Quantitative coronary angiography is unreliable in assessing the severity of jailed side-branch lesions and tends to overestimate the stenosis severity. The likelihood of a side-branch lesion with a <50% ostial stenosis is exceedingly low, and a single stent strategy is preferred in Medina 0,1,0 lesions.1
Pre-intervention physiological assessment has been shown to guide appropriate PCI, with reduced early and late major adverse cardiovascular events compared with angiographic assessment and deferral of PCI with reductions in death and myocardial infarction.2 Nonetheless, post-PCI evaluation is less commonly performed. In the recently presented DEFINE PCI (Physiologic Assessment of Coronary Stenosis Following PCI) trial, iFR post "angiographically successful" PCI was 0.93 ± 0.07 with almost 1 in 4 patients (24%) having iFR < 0.90. Low post-PCI iFR was related to reference vessel diameter and left anterior descending artery (LAD) location, but not degree of angiographic stenosis (<50% vs. ≥50%).2 This suggests that angiography is as unreliable for evaluating functional severity post-PCI as it is pre-PCI (answer A).
Suboptimal post-PCI physiology, even at levels above those associated with ischemia, has been associated with worse outcomes, including more major adverse cardiac events, death, myocardial infarction, and revascularization.3-5
Causes of low post-PCI iFR/FFR include problems with the stent (incomplete expansion and plaque protrusion), stent edge complications (geographical miss, edge dissection, and plaque shift at stent edge), or diffuse disease before and/or after the stent. In the DEFINE-PCI study, the vast majority (82%) of the 24% of patients with iFR ≤ 0.89 after angiographically successful PCI had focal disease on iFR pullback that could be potentially addressed. Further treatment to this focal disease may thus reduce the rate of residual ischemia from 24% to less than 5%. Reduced iFR/FFR after PCI is more likely in LAD lesions, if there is diffuse disease or if the pre-PCI FFR is low.6 Because pre-PCI iFR was particularly low (0.44) in this case, post-PCI evaluation instead of angiography is reasonable (answer C) to assess optimal stent deployment.
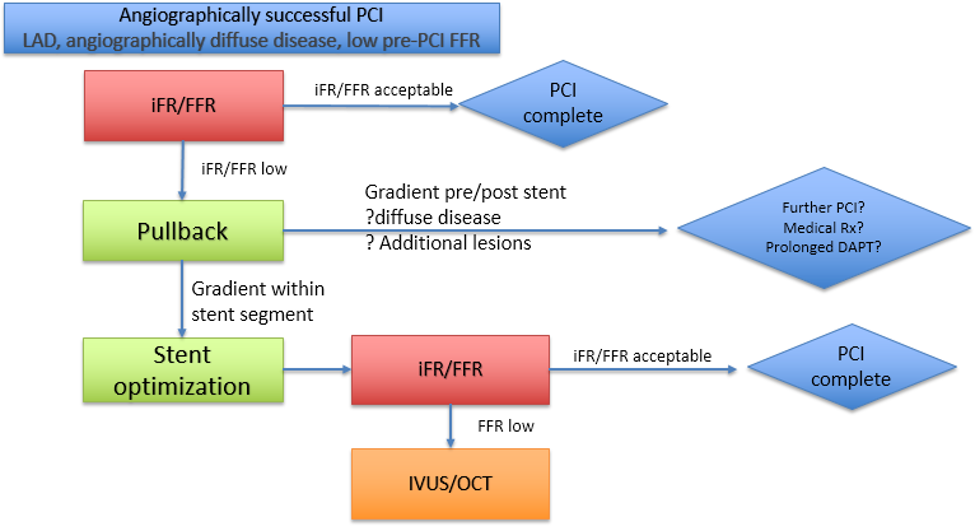
Post-PCI physiologic evaluation with pullback can be used to evaluate for residual focal remote, focal in-stent segment, or diffuse disease. Pullback iFR post-PCI is a quick screening tool to evaluate PCI result that is particularly economically rational if pressure wire assessment is performed prior to PCI; it can also be used to guide stent optimization or further stent placement. Focused intravascular imaging with intravascular ultrasound (IVUS) or OCT can be used to further guide these interventions, and it is reasonable to evaluate the stent segment in focal disease. However, it may be difficult to identify occult hemodynamically significant focal or diffuse disease in the non-stented segment (answer D). We propose the following algorithm (Figure 4) for post-PCI assessment.
Figure 4
Figure 4
In this patient's case, post-stent iFR in the distal LCx was 0.92 with the pullback gradient limited to within the stent. The stent was further dilated using a 3.5 mm non-compliant balloon at 18 atm in its mid and proximal segments, guided by proximal reference measurements on OCT imaging. Final LCx iFR was near-normal at 0.98. The patient subsequently underwent successful transfemoral transcatheter aortic valve replacement with resolution of symptoms and no major adverse cardiovascular events at 30 days and 1-year follow-up after the interventions.
References
Ahn JM, Lee JY, Kang SJ, et al. Functional assessment of jailed side branches in coronary bifurcation lesions using fractional flow reserve. JACC Cardiovasc Interv 2012;5:155-61.
Jeremias A, et al. The DEFINE PCI Trial: Blinded Physiological Assessment of Residual Ischemia after Successful Angiographic Percutaneous Coronary Intervention, presented at American College of Cardiology 2019 Scientific Sessions.
Pijls NH, Klauss V, Siebert U, et al. Coronary pressure measurement after stenting predicts adverse events at follow-up: a multicenter registry. Circulation 2002;105:2950-4.
Wolfrum M, Fahrni G, de Maria GL, et al. Impact of impaired fractional flow reserve after coronary interventions on outcomes: a systematic review and meta-analysis. BMC Cardiovasc Disord 2016;16:177.
Agarwal SK, Kasula S, Hacioglu Y, Ahmed Z, Uretsky BF, Hakeem A. Utilizing Post-Intervention Fractional Flow Reserve to Optimize Acute Results and the Relationship to Long-Term Outcomes. JACC Cardiovasc Interv 2016;9:1022-31.
Agarwal SK, Kasula S, Almomani A, et al. Clinical and angiographic predictors of persistently ischemic fractional flow reserve after percutaneous revascularization. Am Heart J 2017;184:10-6.