A 28-year-old woman with a past medical history of systemic lupus erythematosus (SLE) presented with 1.5 years of shortness of breath and left-sided pleuritic chest pain. Her previous manifestations of SLE included joint inflammation, pleuritis, and shrinking lung syndrome. During a hospital admission for shortness of breath one year prior, she was found to have reaccumulation of bilateral pleural effusions despite prior drainage. As a result, she underwent left-sided video-assisted thoracoscopic surgery and pleural biopsy, which showed chronic pleuritis. During that admission, she was also found to have a trace pericardial effusion with no tamponade physiology. After discharge, her symptoms of shortness of breath and left-sided pleuritic chest pain persisted, and she was unable to exercise or work. The following year, she was referred to a cardiologist for reassessment of her previously-seen trace pericardial effusion.
Her medications included mycophenolate mofetil 1,000 mg PO BID, hydroxychloroquine 400 mg PO daily, amlodipine 5 mg PO daily, cholecalciferol 50,000 units q weekly, and recently completed prednisone taper of 1.5 years' duration for treatment of her pleuritis/serositis and joint inflammation.
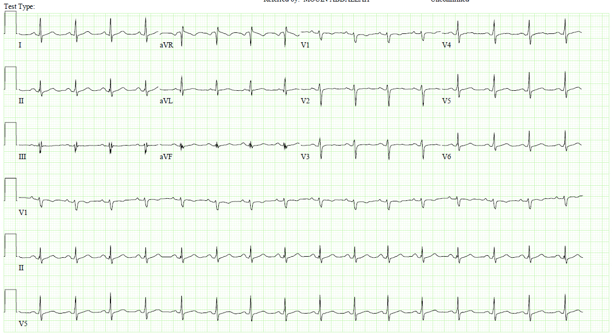
On physical examination, blood pressure was 137/90, heart rate 63 beats per minute, oxygen saturation was 100% on room air, and body temperature was 36.5 degrees Celsius. There was no pulsus paradoxus present. There was no rub or knock present on cardiac auscultation. There was no ascites or peripheral edema. Laboratory investigations showed C-reactive protein 0.2 (< 0.9 mg/dL), ultrasensitive C-reactive protein 2.0 (< 3.1 mg/L), erythrocyte sedimentation rate 10 (0-20 mm/hr). Electrocardiogram was obtained.
Figure 1
Figure 1
Electrocardiogram demonstrated sinus rhythm with no ST segment changes.
Electrocardiogram demonstrated sinus rhythm with no ST segment changes.
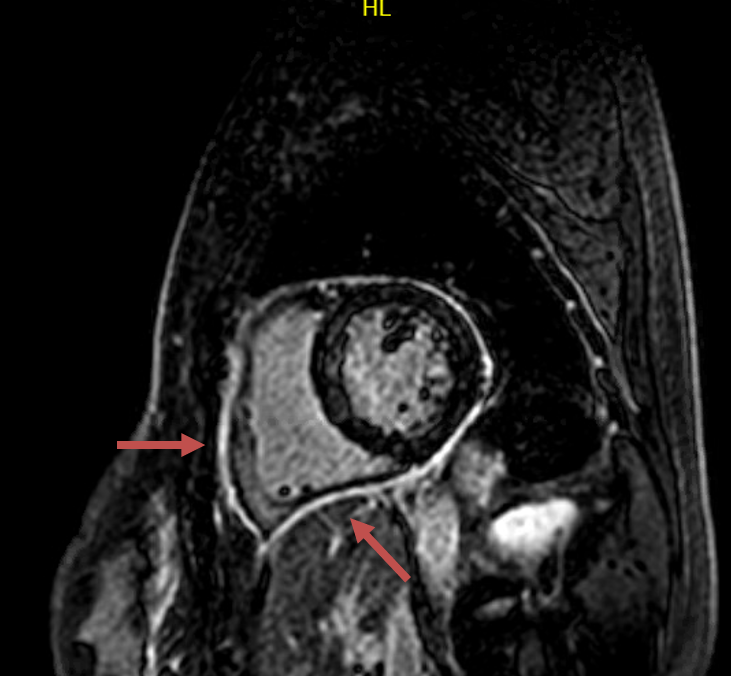
Repeat echocardiogram revealed preserved left ejection fraction but did not demonstrate a pericardial effusion. Cardiac magnetic resonance imaging (CMR) study was performed and revealed acute and subacute pericardial inflammation.
Figure 2
Figure 2
CMR showed moderate circumferential pericardial delayed enhancement (arrows) compatible with pericardial inflammation. There was trivial pericardial effusion with no pericardial thickening. No findings were present to suggest constrictive pericarditis. Specifically, there was no respirophasic septal shift, though subtle diastolic septal bounce was present. There was no diastolic restraint or conical deformity of the ventricles.
CMR showed moderate circumferential pericardial delayed enhancement (arrows) compatible with pericardial inflammation. There was trivial pericardial effusion with no pericardial thickening. No findings were present to suggest constrictive pericarditis. Specifically, there was no respirophasic septal shift, though subtle diastolic septal bounce was present. There was no diastolic restraint or conical deformity of the ventricles.
Figure 3
Figure 3
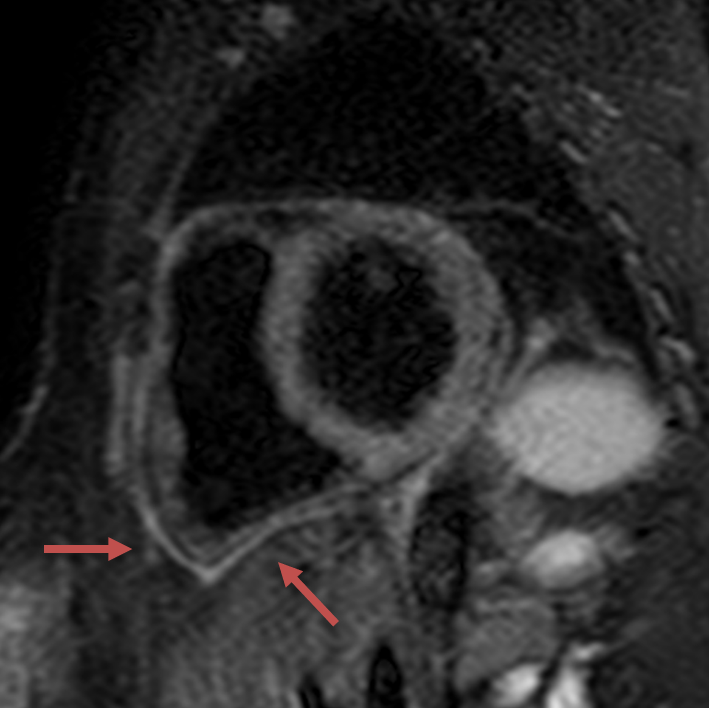
Focal increased anterior pericardial signal intensity on T2 STIR imaging, consistent with pericardial inflammation.
Focal increased anterior pericardial signal intensity on T2 STIR imaging, consistent with pericardial inflammation.
What is the management of this patient's presentation of acute pericarditis?
Show Answer
The correct answer is: D. Start colchicine and restart prednisone
Pericardial manifestations of autoimmune diseases most frequently include asymptomatic pericardial effusions and acute pericarditis, while other manifestations such as constrictive pericarditis and tamponade are uncommon.1,2 Pericardial disease rarely occurs as the first indicator of autoimmune disease, and it often arises in the setting of other types of serositis such as pleuritis.3,4 The development of pericardial disease in patients with known chronic autoimmune conditions is generally presumed to be caused by the existing autoimmune process, and may also signify an ongoing flare of the patient's autoimmune disease.4 Unless other etiologies are suspected, a definitive histologic diagnosis is not usually pursued. Presence of antibodies in the pericardial fluid usually reflects the levels present in the peripheral blood, and therefore is of little utility in diagnosis and management. Immune complex deposition may be present in the pericardium upon biopsy.5
The diagnosis of acute pericarditis can be challenging in the setting of systemic autoimmune disease. Patients are often already on immunosuppressive medications which may blunt the rise of inflammatory markers typically seen in acute pericarditis. At the time of presentation, this patient had been on chronic immune-modulating drugs, which may have led to the normalization of her inflammatory markers without adequately addressing the disease activity present in the pericardium. Conversely, in other patients, it may be impossible to distinguish whether an elevation of inflammatory markers is related to pericardial injury, or instead, autoimmune disease affecting organ systems located elsewhere. Other features of pericarditis such as a pericardial friction rub and electrocardiographic changes may or may not be present. As a result, a thorough intake of the patient's history of presenting illness specifically directed towards eliciting the nature and severity of symptoms consistent with pericarditis is important. Ancillary imaging such as CMR is useful in verifying the presence and severity of pericardial inflammation. Inflamed tissue caused by acute pericarditis appears bright and thickened on T2-weighted images, findings which represent edema. With CMR, late gadolinium enhancement also denotes inflammation, and furthermore, can help prognosticate a patient's clinical course with respect to remission, recurrence rate, and time to recurrence.6
Management of autoimmune-related pericardial injury is dependent upon the presence of symptoms. If the patient is asymptomatic, then the treatment is the same as that of the patient's systemic disease. (Answer A) Conversely, if the patient has symptoms, as in the case of autoimmune pericarditis illustrated above, then intensification of the patient's immunosuppressive therapy is warranted. In contrast to viral or idiopathic pericarditis, in which non-steroidal anti-inflammatories (NSAIDs) are part of the first-line treatment (Answer B), glucocorticoids are preferred among patients with autoimmune pericarditis.7 (Answer D) In this patient, the initiation of glucocorticoids is warranted in addition to the continuation of the immunosuppressive medications that are already being used to control the other systemic manifestations of SLE. It is important to note that the patient's aforementioned imaging findings are relevant in the discussion of her treatment strategy and in anticipating her response to therapy. A protracted clinical course is likely based on the presence of the moderate degree of delayed gadolinium hyperenhancement seen on CMR.6 Therefore, a long treatment period involving a slow taper of prednisone is to be expected.
The use of colchicine in isolation is unlikely to be sufficient in adequately treating the patient's SLE-related pericarditis given her symptoms and radiographic abnormalities. (Answer C) In general, the use of colchicine as an adjunct therapy in autoimmune pericarditis has not been studied extensively. However, in clinical practice, the addition of colchicine to immunosuppressive therapy such as glucocorticoids is commonly implemented based on the extrapolation of data regarding its benefit observed in cases of acute and recurrent pericarditis.8 As a result, this patient was treated with a dual therapy regimen consisting of the concurrent resumption of a prednisone taper and initiation of colchicine. (Answer D)
References
Langley RL, Treadwell EL. Cardiac tamponade and pericardial disorders in connective tissue diseases: case report and literature review. J Natl Med Assoc 1994;86:149-53.
Doria A, Iaccarino L, Sarzi-Puttini P, Atzeni F, Turriel M, Petri M. Cardiac involvement in systemic lupus erythematosus. Lupus 2005;14:683-86.
Man BL, Mok CC. Serositis related to systemic lupus erythematosus: prevalence and outcome. Lupus 2005;14:822-26.
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Jacobson EJ, Reza MJ. Constrictive pericarditis in systemic lupus erythematosus. Demonstration of immunoglobulins in the pericardium. Arthritis Rheum 1978;21:972-74.
Kumar A, Sato K, Yzeiraj E, et al. Quantitative pericardial delayed hyperenhancement informs clinical course in recurrent pericarditis. JACC Cardiovasc Imaging 2017;10:1337-46.
Cremer PC, Kumar A, Kontzias A, et al. Complicated pericarditis: understanding risk factors and pathophysiology to inform imaging and treatment. J Am Coll Cardiol 2016;68:2311-28.
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation 2005;112:2012-16.