A 49-year-old female with a history of premature atrial and ventricular complexes and hypertension presented to the cardiology clinic for progressive dyspnea and exertional fatigue. On presentation, her heart rate was within normal limits, with a blood pressure of 130/80 mmHg, and room air saturations of 98%. Cardiac auscultation revealed a regular rhythm and a 2/6 systolic murmur at the lower left sternal border. An echocardiogram (Figure 1) revealed a flattened septum and dilation of the right atrium and ventricle. There was mild mitral valve prolapse with mild mitral regurgitation, moderate tricuspid regurgitation and an estimated right ventricular systolic pressure (RVSP) of less than ½ systemic. There was no evidence of an interatrial shunt in technically difficult, limited views.
Figure 1
Figure 1
Figure 1: 4 chamber view
Figure 1: 4 chamber view
Transesophageal echocardiogram (TEE) revealed a non-stenotic pulmonary valve with mild pulmonary insufficiency, a normal left ventricular ejection fraction, and a dilated right ventricle. The atrial septum was intact.
What is the cause of dyspnea and right ventricular dilatation in this patient?
Show Answer
The correct answer is: C. Anomalous pulmonary venous drainage
Cardiac magnetic resonance imaging confirmed this diagnosis (Figures 2-4).
Figure 2
Figure 2
Figure 2: 4-Chamber SSFP; Right ventricular enlargement
Figure 2: 4-Chamber SSFP; Right ventricular enlargement
Figure 3
Figure 3
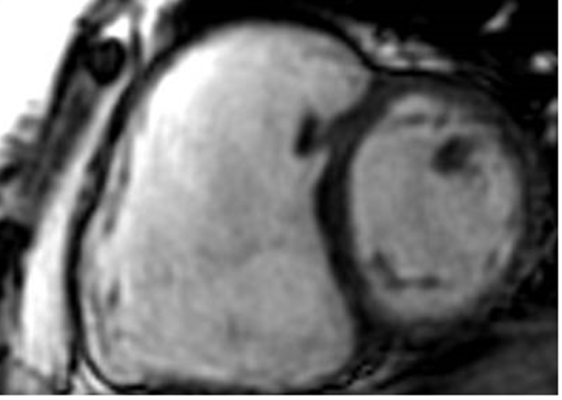
Figure 3: Short Axis; Right ventricular enlargement with apparent volume overload
Figure 3: Short Axis; Right ventricular enlargement with apparent volume overload
Figure 4
Figure 4
Figure 4: 3-D reconstruction of a time resolved MRA
Anomalous right upper pulmonary vein with drainage into the superior vena cava. Qp/Qs is 2.0. No evidence of an accompanying sinus venosus atrial septal defect.
Figure 4: 3-D reconstruction of a time resolved MRA
Anomalous right upper pulmonary vein with drainage into the superior vena cava. Qp/Qs is 2.0. No evidence of an accompanying sinus venosus atrial septal defect.
Dilation of the right ventricle (RV) may be seen on transthoracic echocardiograms (see Figure 1) and can be associated with a variety of clinical disorders. In the absence of valvular heart disease, the differential diagnosis includes pulmonary hypertension as well as a variety of congenital defects associated RV volume or pressure over-load. These defects include total anomalous pulmonary venous return (TAPVR), partial anomalous pulmonary venous return (PAPVR), large atrial septal defects (ASD), as well as large coronary artery to right heart fistulae.
TAPVR is a rare congenital condition affecting 0.6 to 1.2 per 10,000 live births. It occurs when all the pulmonary veins drain into the right atrium instead of the left atrium, resulting in cyanosis. It is usually diagnosed shortly after birth.1 This is unlikely in an adult patient with normal oxygen saturation.
PAPVR occurs when some of the pulmonary veins drain into the right atrium or superior vena cava instead of the left atrium. PAPVR is more common, and likely underdiagnosed, estimated to affect 0.7% of the population.2 PAPVR involving the right superior pulmonary vein is frequently associated with a sinus venosus atrial septal defect.3 The ratio of pulmonary blood flow (Qp) to systemic blood flow (Qs) (Qp:Qs ratio) quantifies the shunt and its clinical implications. The number of anomalous pulmonary veins determines the magnitude of the shunt. An associated ASD may exacerbate RV volume overload.4 The normal Qp:Qs ratio is 1:1 and ratios above 2:1 are considered large enough to have long-term hemodynamic and clinical implications. After years of excessive RV volume overload, these large shunts result in dilatation of the right atrium and right ventricle and can lead to pulmonary hypertension, right heart failure, and arrhythmias.
Surgery is indicated to correct the significant volume load to the RV once recognized. The cardiac magnetic resonance imaging (MRI) in this patient revealed an anomalous right upper pulmonary vein draining into the superior vena cava, with an intact atrial septum. The Qp:Qs ratio was 2.0. with a severely dilated right ventricular cavity and mildly reduced right ventricular systolic function.
The patient was referred for surgical correction, which revealed a right superior and middle pulmonary vein draining into the right atrium. The atrial septum was intact. An atrial septal incision was made and a baffle created that allowed the pulmonary veins to drain into the left atrium. A patch was then placed over the superior venae cavae venotomy sites. The patient recovered uneventfully.
Ellis A. "Partial Anomalous Pulmonary Venous Connections and the Scimitar Syndrome." In: Gatzoulis MA, Webb GD, eds. Diagnosis and Management of Adult Congenital Heart Disease, 3rd ed. Philadelphia, PA: Elsevier;2018:354-61.
Bernstein D. "Acyanotic Congenital Heart Disease: Left to Right Shunt Lesions. Partial Anomalous Pulmonary Venous Return." In: Kliegman RM, St. Geme, J, eds. Nelson Textbook of Pediatrics, 20th ed. Philadelphia, PA: Elsevier;2016:2189-99.
Seller N, Yoo SJ, Grant B, Groose-Wortmann L. How many versus how much: comprehensive haemodynamic evaluation of partial anomalous pulmonary venous connection by cardiac MRI. Eur Radiol 2018;28:4598-4606.