A 75-year-old male patient with a history of systolic heart failure presented with worsening dyspnea (New York Heart Association Class 3 versus 2 at previous visit). On physical examination, his blood pressure was 125/79 mmHg, and he had a rough systolic murmur with blunted S2 in the aortic area. His pulmonary auscultation was normal, and there were no signs of congestion. On echocardiography, the left ventricle showed global hypokinesia, and the left ventricular ejection fraction (LVEF) was 40%. The aortic valve appeared thickened with reduced opening (Video 1).
Video 1
Video 1
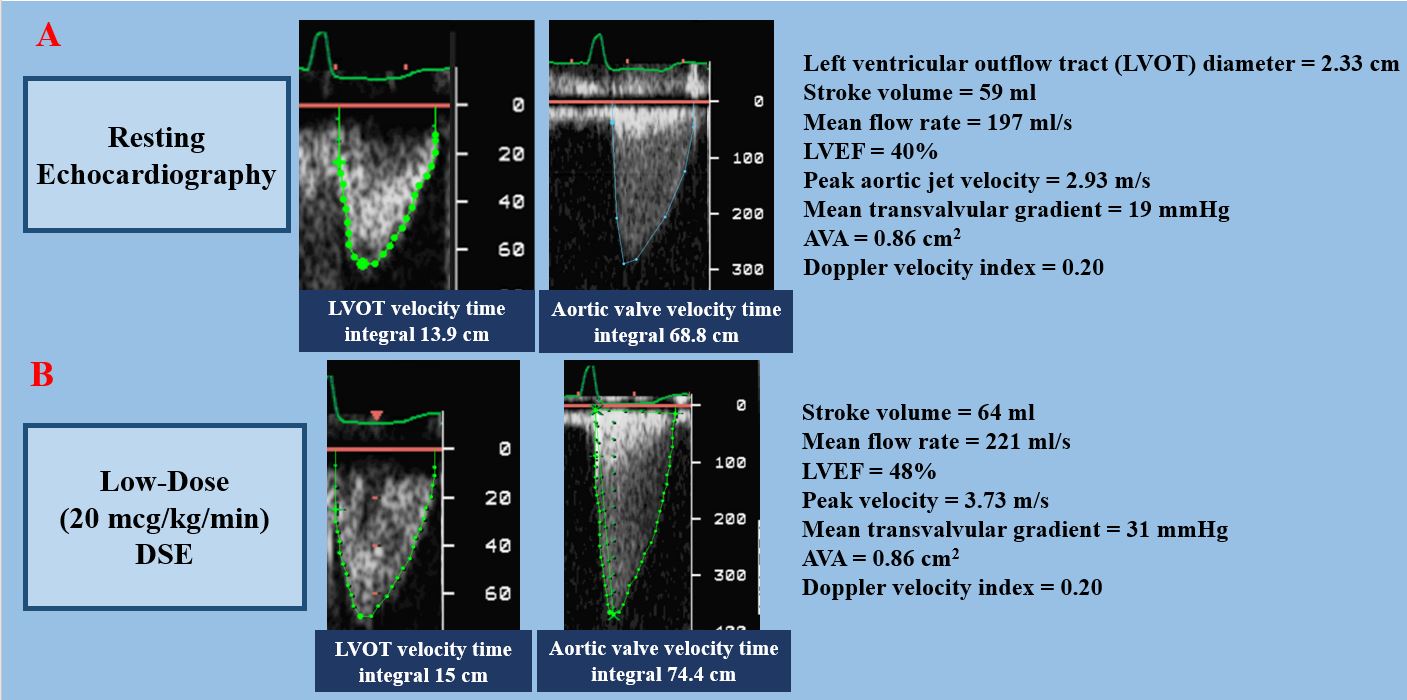
The transvalvular mean gradient (MG) and peak aortic jet velocity were 19 mmHg and 2.93 m/s, respectively, and the aortic valve area (AVA) was calculated at 0.86 cm2 with a stroke volume of 59 ml/beat (i.e. 28 ml/m2 when indexed to body surface area) (Figure 1A); the mean flow rate was 197 ml/s. The patient underwent low-dose (i.e., 20 mcg/kg/min) dobutamine stress echocardiography (DSE) (Figure 1B) to confirm severity of aortic stenosis (AS). At peak dobutamine stress, the MG, peak aortic velocity, and AVA were 31 mmHg, 3.73 m/s, and 0.86 cm2, respectively, with a stroke volume of 64 ml (30 ml/m2) and a mean flow rate of 221 ml/s.
Figure 1
Figure 1
What is the severity of the AS, and what are the next steps in the management of this patient?
Show Answer
The correct answer is: D. Indeterminate AS severity; perform aortic valve calcium score using non-contrast multidetector computed tomography (MDCT) and treat with AVR if true-severe AS is confirmed
In this patient with low-LVEF, low-flow, low-gradient AS, the grading of AS severity is discordant at resting echocardiography: the AVA is <1.0 cm2, suggesting severe AS, but the MG is <40 mmHg, suggesting non-severe AS.1 The MG is highly flow-dependent and may thus underestimate the AS severity in the context of low-flow state, whereas the AVA may overestimate the severity.
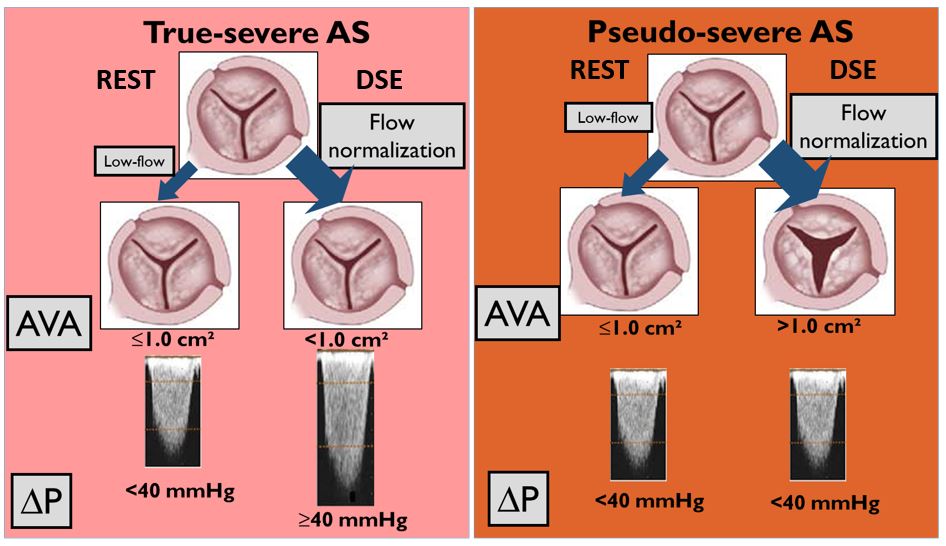
The distinction of true- versus pseudo-severe AS is crucial for therapeutic decision-making. This can be achieved using low-dose DSE (i.e., 20 mcg/kg/min) (Figure 2). If MG reaches the severity cut-point of 40 mmHg and AVA remains below 1.0 cm2 with DSE-induced increase in flow, the stenosis is considered true-severe.1 However, in this patient, the discordance between AVA (<1.0 cm2) and MG (<40 mmHg) persisted at DSE because there was no significant increase in flow (i.e., no flow reserve). This situation occurs in approximately one third of the patients,2 and in such cases, AS severity remains indeterminate with DSE. Therefore, answers A and B are incorrect.
Figure 2
Figure 2
In patients with limited (but still present) flow reserve, the flow increases but remains below normal. In this situation, the AVA-MG discordance may persist at the end of DSE. However, if there is at least 15% increase in mean flow rate (stroke volume/left ventricular ejection time), it is possible to calculate the projected AVA at normal flow rate (250 ml/s) to confirm AS severity.2 In this case, the patient had no significant increase in stroke volume or flow rate; thus, it is thus not possible to obtain a reliable estimate of the projected AVA. Therefore, answer E is incorrect.
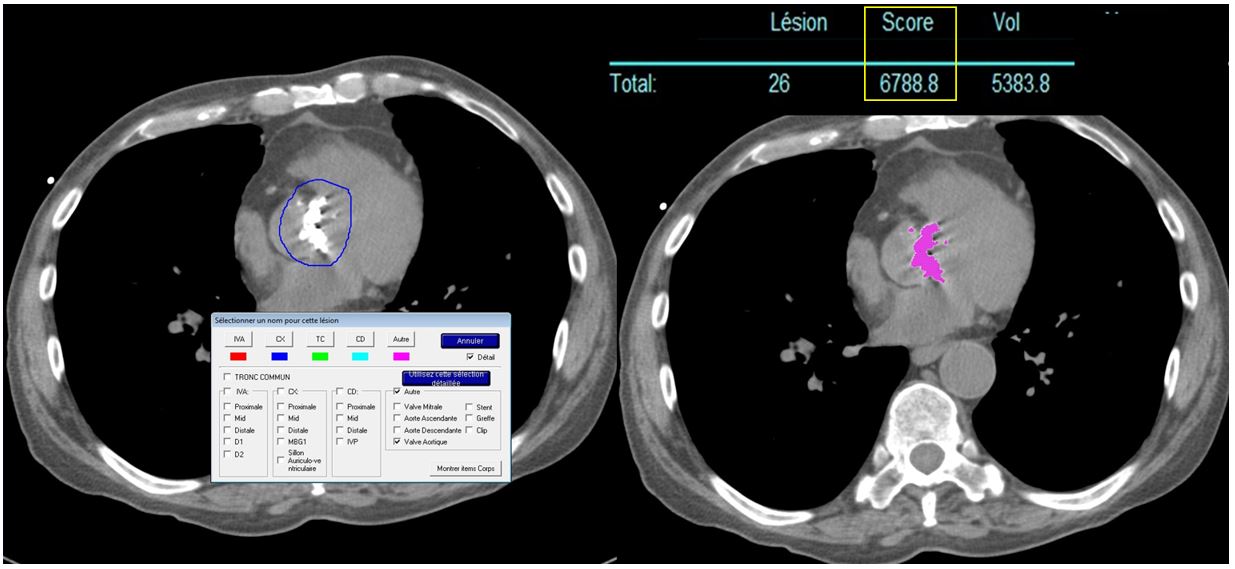
In this patient with inconclusive DSE, the next step is to quantify the aortic valve calcium using non-contrast MDCT (Figure 3). This approach has been shown to be accurate to distinguish true-severe from pseudo-severe AS3 and to predict patient outcome4 and has recently been recommended in the 2017 European guidelines for the management of valvular heart disease.5 Therefore, answer D is correct and answer C is incorrect. The calcium score in this patient is 6,788 AU (Figure 3), which is markedly higher than the recommended cut-point for severe AS in men (2,000 AU).5 This confirms the presence of true-severe AS and the indication of AVR. The absence of flow reserve on DSE is a marker for high operative risk with surgical AVR6 and may thus be considered as an argument to select transcatheter rather than surgical AVR in this patient.7
Figure 3
Figure 3
References
Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017;70:252-89.
Annabi MS, Touboul E, Dahou A, et al. Dobutamine Stress Echocardiography for Management of Low-Flow, Low-Gradient Aortic Stenosis. J Am Coll Cardiol 2018;71:475-85.
Clavel MA, Messika-Zeitoun D, Pibarot P, et al. The complex nature of discordant severe calcified aortic valve disease grading: new insights from combined Doppler echocardiographic and computed tomographic study. J Am Coll Cardiol 2013;62:2329-38.
Clavel MA, Pibarot P, Messika-Zeitoun D, et al. Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aortic stenosis: results of an international registry study. J Am Coll Cardiol 2014;64:1202-13.
Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2017;38:2739-91.
Tribouilloy C, Lévy F, Rusinaru D, et al. Outcome after aortic valve replacement for low-flow/low-gradient aortic stenosis without contractile reserve on dobutamine stress echocardiography. J Am Coll Cardiol 2009;53:1865-73.
Ribeiro HB, Lerakis S, Gilard M, et al. Transcatheter Aortic Valve Replacement in Patients With Low-Flow, Low-Gradient Aortic Stenosis: The TOPAS-TAVI Registry. J Am Coll Cardiol 2018;71:1297-308.