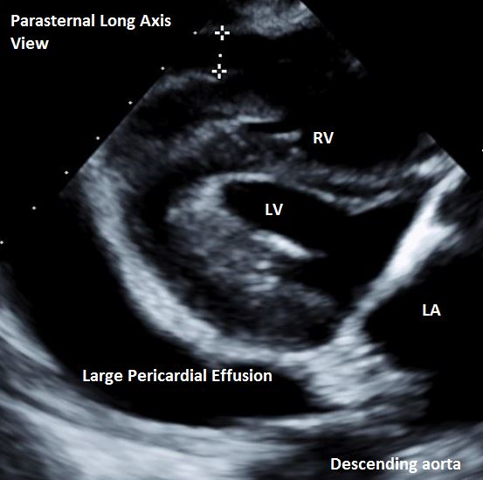
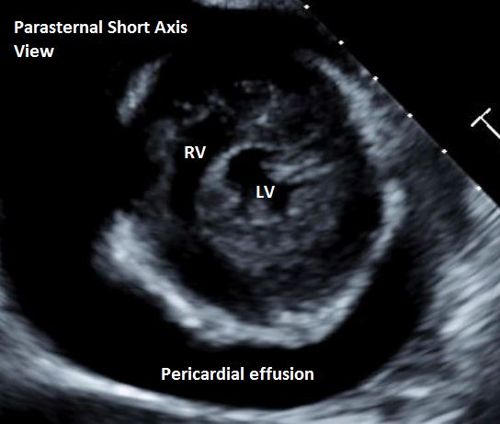
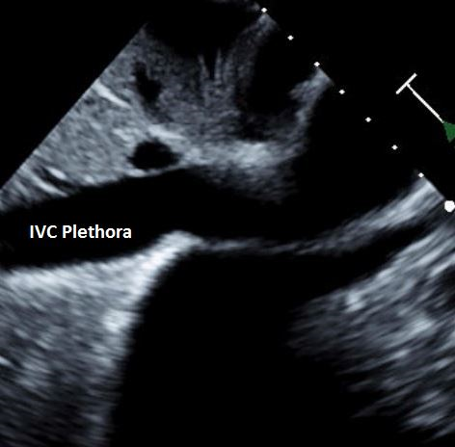
A 69-year-old female with a past medical history of severe aortic stenosis, heart failure with preserved ejection fraction and paroxysmal atrial fibrillation on rivaroxaban and diltiazem presented to the emergency department with shortness of breath and lightheadedness. Her vital signs were significant for hypotension. Cardiovascular examination revealed muffled heart sounds and an elevated jugular venous pressure. An electrocardiogram was done which showed atrial fibrillation with rapid ventricular response. The echocardiogram revealed a large pericardial effusion (Image 1 and Image 2) and plethora of the inferior vena cava (Image 3). M mode showed diastolic collapse of the right ventricle. Doppler interrogation of mitral inflow showed >30% change in velocity with respiration. Pericardiocentesis was performed with removal of 650 milliliters of bloody fluid. Her symptoms resolved. Analysis of the pericardial fluid revealed 1.5 million RBCs/μl and 5700 WBCs/μl with 74% neutrophils, 16% lymphocytes and 10% monocytes. Cytology was negative for malignant cells. Repeat echocardiogram showed resolution of the pericardial fluid. Of note, she did not have a prior history of a pericarditis or previous cardiac procedure.
Image 1: Parasternal Long Axis View
Image 1
Image 2: Parasternal Short Axis View
Image 2
Image 3: IVC Plethora
Image 3
Which of the following predisposed the patient to develop a hemorrhagic pericardial effusion?
Show Answer
The correct answer is: D. Receiving diltiazem along with rivaroxaban
The patient had a spontaneous hemorrhagic tamponade likely due to increased plasma concentration of rivaroxaban and underwent a pericardiocentesis to drain the hemopericardium.1 On many occasions, it is difficult to decide between using a needle for pericardiocentesis versus surgery/pericardial window to drain the hemopericardium. A single-center retrospective study showed that echocardiography-guided needle pericardiocentesis in tamponade resulted in fewer complications and a lower mortality rate when compared to a surgical approach.2 Another single-center retrospective study, however, showed that there was no statistically significant difference in mortality between surgery versus needle pericardiocentesis (19.8% in the surgical group vs 18.1% in the pericardiocentesis group; p=0.8). Complications like myocardial perforation and perforation of the coronary artery, however, occur at a higher rate when pericardial windows are done (4.9% vs 26.4%; p<0.0001), which may make needle pericardiocentesis more preferable in patients with hemopericardium.3 The 2015 ESC guidelines also recommend that drainage of pericardial fluid in cases of tamponade should be done preferably by needle pericardiocentesis with the use of echocardiographic or fluoroscopic guidance.4
An important point of caution is that in cardiac tamponade that occurs as a complication of aortic dissection, pericardiocentesis may precipitate hemodynamic collapse and death. In such cases, pericardiocentesis should be avoided and the patient should be transferred to the operating room as urgently as possible for surgical repair of the aorta and intraoperative drainage of the hemopericardium. Urgent pericardiocentesis may still be indicated, however, if the blood pressure is too low and vital organ perfusion is compromised, but even in that case, aspiration of only a small amount of pericardial fluid is recommended, just enough to raise the patient's blood pressure to the lowest acceptable value. This minimizes the chances of precipitating a rapid increase in blood pressure, which could induce further extension of the dissection or could also cause the hemorrhage to recur. Hence, in a case of hemopericardium, it is very important to rule out aortic dissection, before making the decision to perform pericardiocentesis.5 In the described case, aortic dissection was ruled out by echocardiography and the hemopericardium was thought to be rivaroxaban-induced in the setting of concurrent use of diltiazem.
Rivaroxaban is an oral direct Factor Xa inhibitor widely used for stroke prevention in patients with non-valvular atrial fibrillation. Unlike warfarin, it is convenient to use, since monitoring its blood level is not required. However, hemorrhage is still one of its major side effects, especially, when combined with other medications that could increase its plasma level. Rivaroxaban is a substrate of the cytochrome P450 enzyme-CYP3A4. Diltiazem is a weak-moderate inhibitor of CYP3A4. Hence, concurrent use of diltiazem with rivaroxaban causes an increased plasma level of rivaroxaban, predisposing the patient to hemorrhagic side effects.6
Hemopericardium with tamponade physiology is an uncommon complication of rivaroxaban use. It is important to consider this diagnosis when patients on rivaroxaban present with symptoms of tamponade especially when there is concurrent use of a CYP3A4 inhibitor such as diltiazem. Some other drugs that are inhibitors of the enzyme are amiodarone, verapamil, dronedarone, conivaptan and certain antifungals, to name a few. Though direct oral anticoagulants (DOACs) are convenient to use, this case illustrates the need to consider drug-drug interactions before prescribing them.
References
Basnet S, Tachamo N, Tharu B, Dhital R, Ghimire S, Poudel DR. Life-threatening hemopericardium associated with rivaroxaban. Case Report 2017;4691325:1–3.
Gumrukcuoglu HA, Odabasi D, Akdag S, Ekim H. Management of cardiac tamponade: a comparative study between echo-guided pericardiocentesis and surgery—a report of 100 patients. Cardiol Res Pract 2011;2011:197838.
Saltzman AJ, Paz YE, Rene AG, et al. Comparison of surgical pericardial drainage with percutaneous catheter drainage for pericardial effusion. J Invasive Cardiol 2012;24:590–93.
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J 2015;36:2921–64.
Isselbacher EM, Cigarroa JE, Eagle KA. Cardiac tamponade complicating proximal aortic dissection. Is pericardiocentesis harmful? Circulation 1994;90:2375–78.
Menendez D, Michel J. Hemopericardium with tamponade following rivaroxaban administration and its attenuation by CYP3A4 inhibitors. Proc (Bayl Univ Med Cent) 2016;29:414–15.