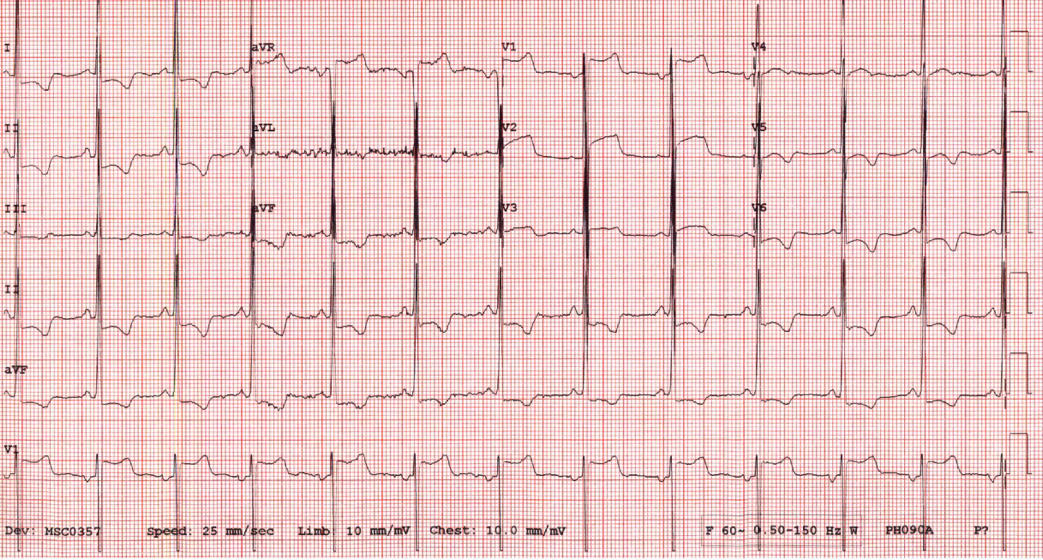
A 20-year old African American male presented with palpitations during a warm-up prior to a training session. He is a freshman in the Air Force Academy and plays power forward on the basketball team. He does not have a significant past medical or family history and does not consume alcohol, stimulants, or anabolic steroids. His blood pressure (BP) was 118/78, pulse 75 bpm, and cardiac examination was unremarkable. Electrocardiogram (ECG) showed left ventricular hypertrophy (LVH) by voltage criteria (Sokolow-Lyon) and deep T-wave inversions in the inferior and lateral leads (Figure 1). Echocardiography showed diffuse concentric LVH (maximal wall thickness:15mm; relative wall thickness 0.65), left ventricle (LV) mass 285gm, left ventricular internal diameter in diastole (LVIDd) 4.3cm, normal left atrial size, normal LV filling and a hyperdynamic ejection fraction of 83%. There was no LV outflow tract obstruction during exercise. An MRI corroborated these findings and post contrast imaging did not demonstrate delayed myocardial enhancement. A 14-day Zio patch recording showed no arrhythmias and genetic testing was negative for pathogenic variants of inherited cardiomyopathies.
Figure 1: 12-lead electrocardiogram (ECG)
Figure 1
Of the following choices, what would be the most reasonable next step?
Show Answer
The correct answer is: B. Maximal exercise testing for arrhythmia provocation
This is a challenging case without a clear answer. Therefore we are unable to definitively diagnose hypertrophic cardiomyopathy (Option D) or athlete's heart (Option E) without further information.1 In this case, the abnormal electrocardiographic findings with a small LV cavity (<45mm) heightens our suspicion for a diagnosis of hypertrophic cardiomyopathy.2 Given the initial presentation with palpitations, it may be most reasonable to next perform a maximal exercise test for arrhythmia provocation (Option B). Although a cardio-pulmonary exercise test would be helpful if the VO2Max is abnormally low (Option A), athletes with hypertrophic cardiomyopathy may have a normal or supra-normal VO2max. Finally, an exercise dose reduction (Option C) to help clarify the diagnosis is controversial, lacking robust supportive evidence, and may not be a viable option for all competitive athletes. However, this strategy, if tolerated, would be a reasonable approach following a maximal exercise test for arrhythmia provocation. For this individual, maximal exercise testing was unremarkable, and he was prepared to reduce exercise levels as he was at the end of the competitive season. While a repeat echocardiogram after an exercise dose reduction did not show any change in LV wall thickness, nearly two years later he developed new discrete upper septal thickening.
References
Wasfy MM, Weiner RB. Differentiating the athlete's heart from hypertrophic cardiomyopathy. Curr Opin Cardiol 2015;30:500–05.
Caselli S, Maron MS, Urbano-Moral JA, Pandian NG, Maron BJ, Pelliccia A. Differentiating left ventricular hypertrophy in athletes from that in patients with hypertrophic cardiomyopathy. Am J Cardiol 2014;114:1383–89.