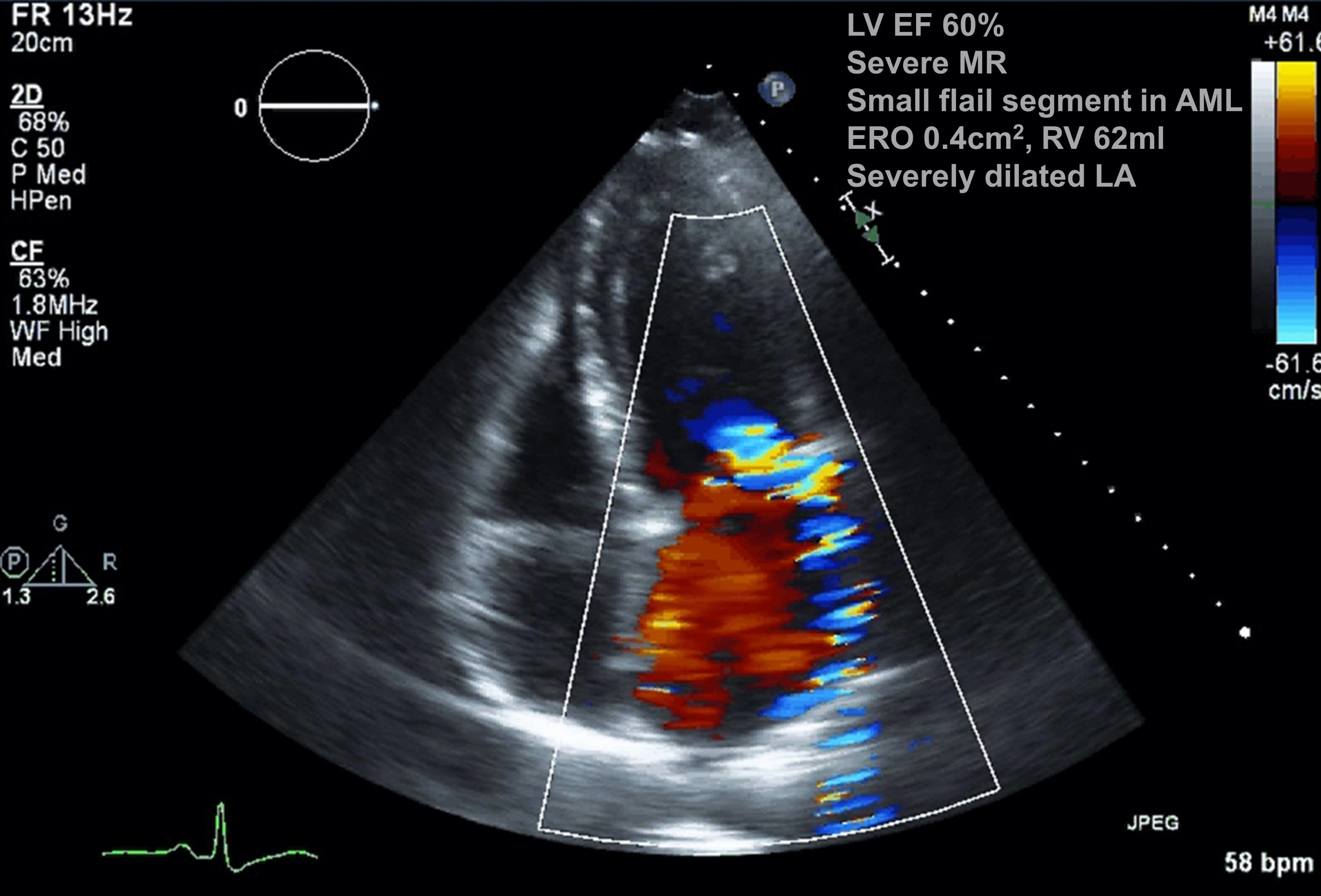
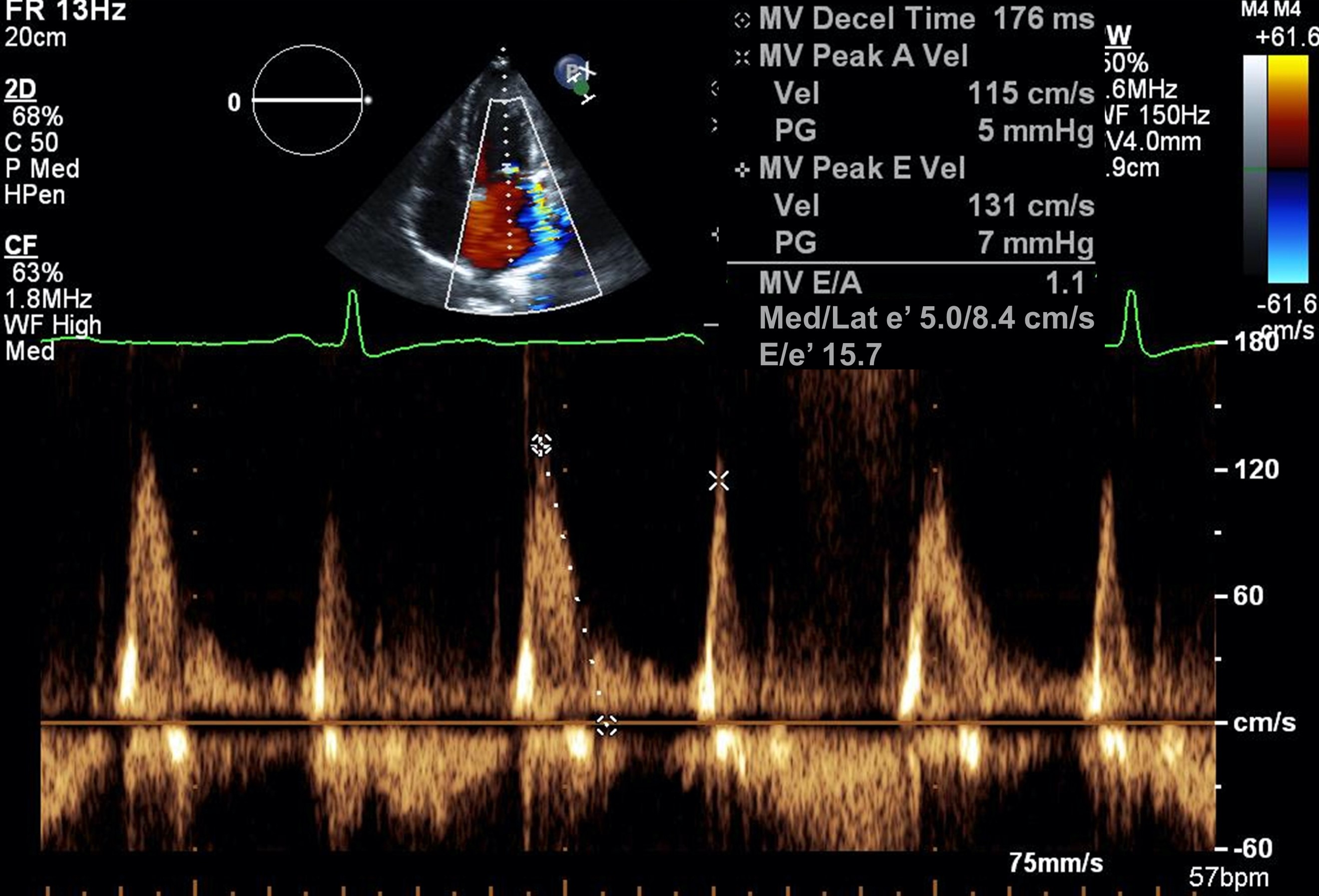
A 77-year-old male patient with a medical history significant for mitral regurgitation (MR), hypertension, diffuse coronary artery disease, and chronic kidney disease stage III was referred for management of chronic systolic and diastolic heart failure. He reported New York Heart Association Class II dyspnea on exertion. The patient's blood pressure was 149/71 mmHg with a heart rate of 60 bpm at rest. An electrocardiogram showed normal sinus rhythm. Transthoracic echocardiography demonstrated severe MR with small flail segment at A2, effective orifice area of 0.4 cm2, regurgitation volume of 62 ml, systolic flow reversal of pulmonary vein, and severely dilated left atrium (LA) (Figure 1). Mitral valve inflow assessment revealed peak E velocity of 131 cm/s, E/A of 1.14, E/e' of 15.7, tricuspid regurgitation velocity of 2.1 m/s, and LA volume index of 52ml/m2 (Figure 2).
Figure 1
Figure 1
Figure 2
Figure 2
How would you grade this patient's degree of diastolic dysfunction?
Show Answer
The correct answer is: D. Cannot determine at this point
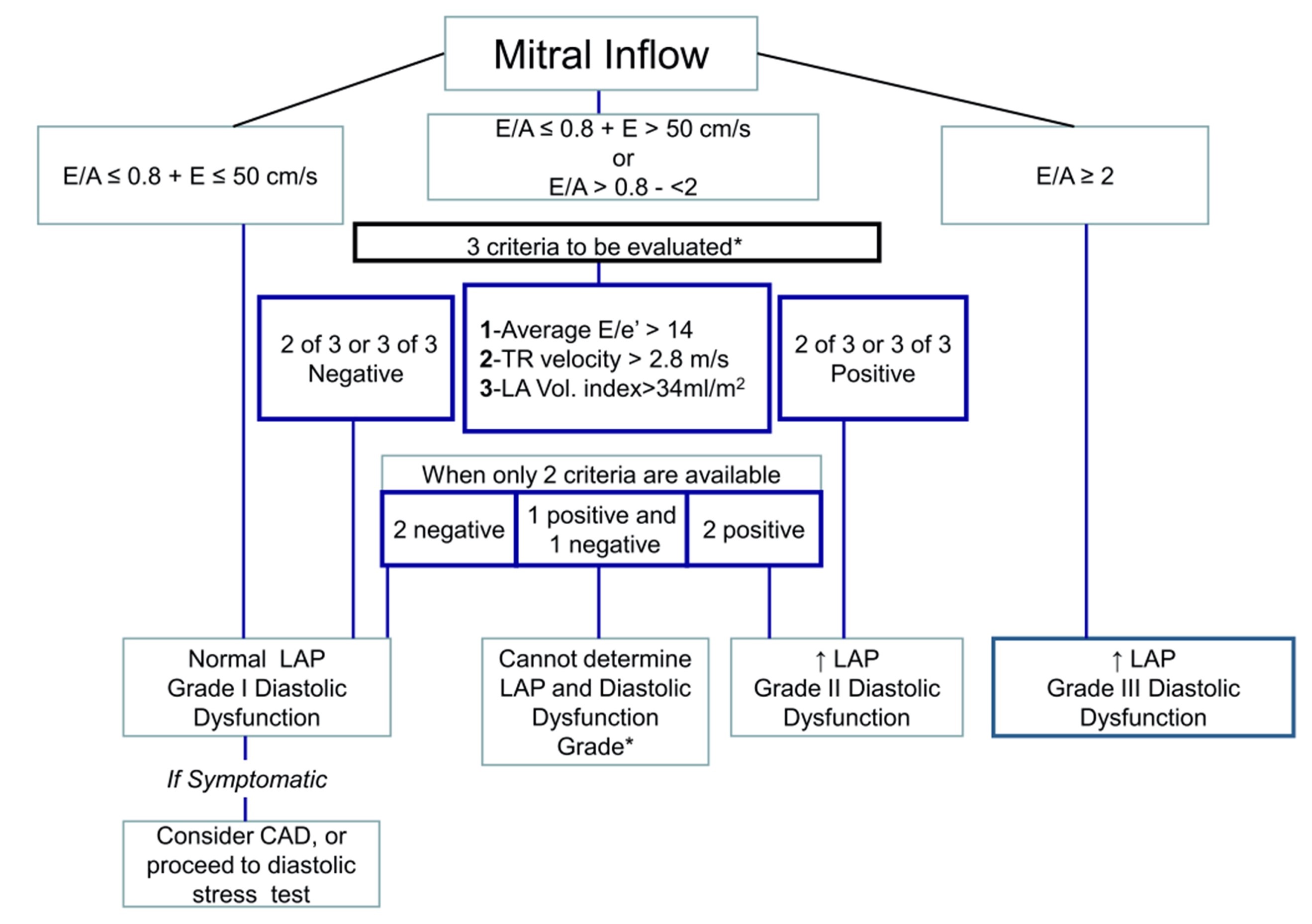
We cannot determine this patient's underlying diastolic dysfunction grade at this point because mitral valve disease may affect his current diastolic dysfunction. Both two-dimensional and Doppler parameters by echocardiography need to be assessed to grade diastolic dysfunction. In addition, the guideline from the American Society of Echocardiography and the European Association of Cardiovascular Imaging stated left ventricular (LV) filling pressure should be estimated because it is strongly related to LV diastolic dysfunction (Figure 3).1
Figure 3
Figure 3
In this case, echocardiographic parameters classified this patient's diastolic dysfunction as grade 2 in the setting of severe MR.
To accurately estimate a patient's degree of diastolic dysfunction, other comorbidities must be considered. Recent guidelines for a comprehensive assessment of diastolic function recommend that each study include an evaluation for underlying cardiomyopathy (hypertrophic and restrictive), valvular disease (MR, mitral stenosis, mitral annular calcification, aortic stenosis, and aortic insufficiency), heart transplantation, and arrhythmia (atrial fibrillation, heart block, and pacing). These conditions each impact LV filling pressures differently. For example, primary MR (this case) leads to LA and LV enlargement and an increase in the compliance of both chambers, which attenuates the increase in LA pressure. With LV diastolic dysfunction, a myocardial component of increased filling pressures is added over time. The sequence is the opposite of that seen in primary myocardial disease such as dilated cardiomyopathy, which leads to increased filling pressures earlier on and later to functional MR. Therefore, in patients with secondary MR, echocardiographic correlates of increased filling pressures reflect the combination of both myocardial and valvular disorders.
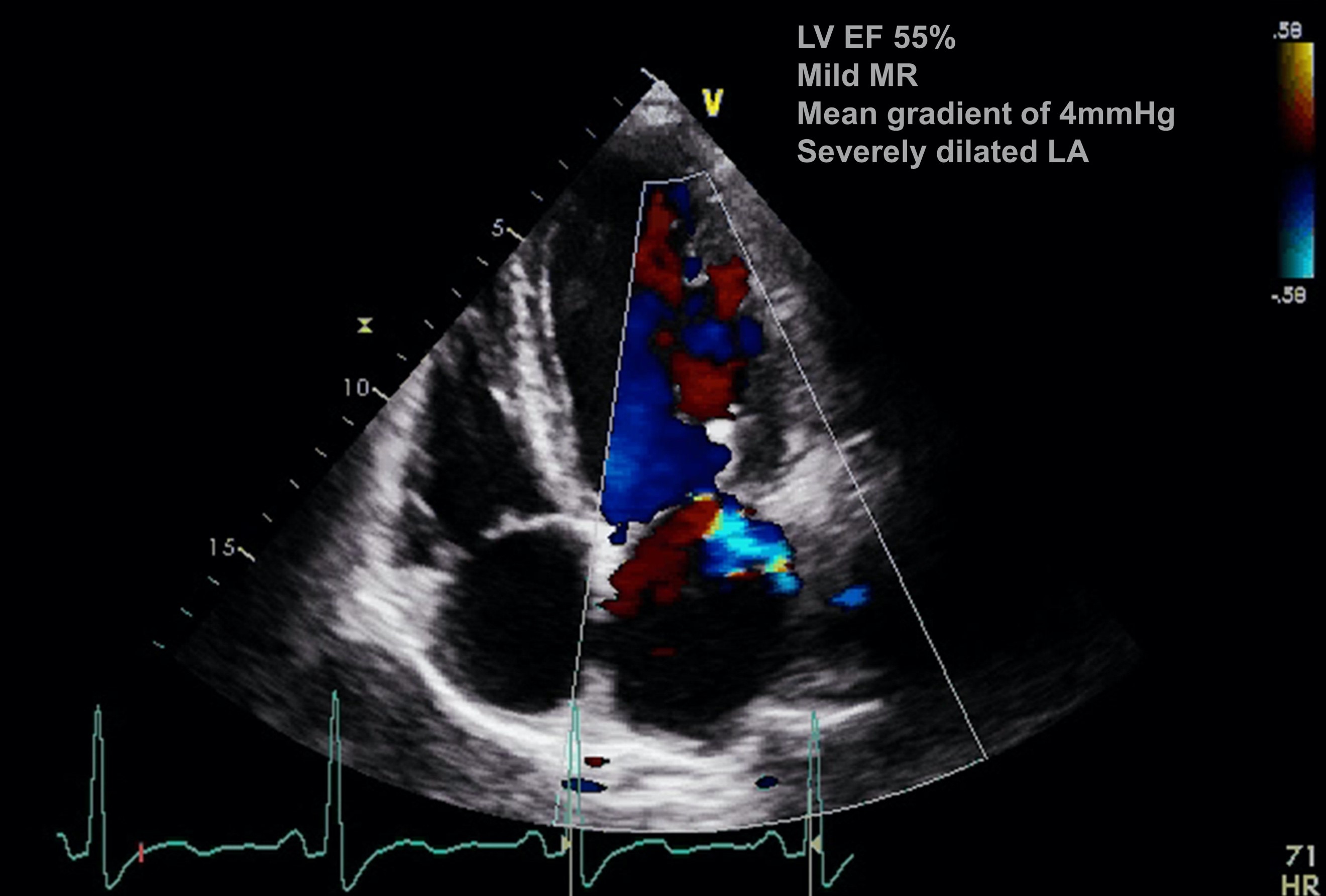
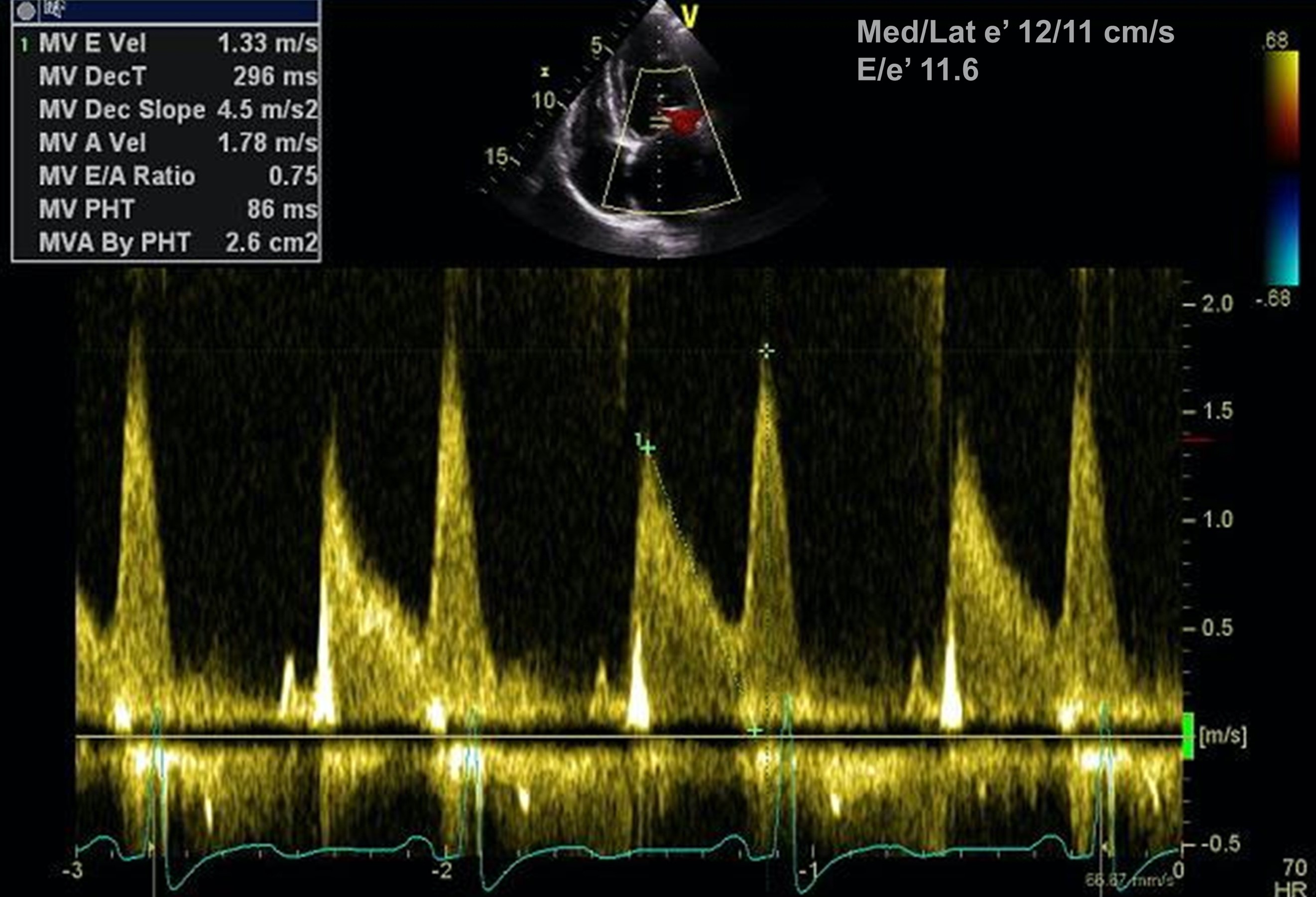
In fact, this patient underwent MitraClip (Abbott; Abbott Park, IL) procedure, reducing MR grade to mild with normalization of systolic flow of pulmonary vein. A 1-year follow-up transthoracic echocardiogram showed peak E velocity of 133 cm/s, E/A of 0.75, E/e' of 11.6, tricuspid regurgitation velocity of 0.96 m/s, and LA volume index of 55 ml/m2, suggesting normal LA pressure and grade 1 diastolic dysfunction (Figures 4-5). This change in diastolic dysfunction grade suggested that MR significantly impacted his diastolic dysfunction.
Figure 4
Figure 4
Figure 5
Figure 5
References
Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2016;29:277-314.