A 45-year-old female presents with chest pressure and dyspnea at rest for two days, followed by a syncopal episode. Her medical history is significant for obstructive sleep apnea, and former tobacco and alcohol abuse (3-4 drinks per day, quit 5 years ago).
Prior to her admission (about 1 year), she presented to her local primary care physician complaining of palpitations, fatigue and low blood pressure readings (BP range 96/70 – 100/70mmHg; HR 80 – 90bpm).
Laboratory work up at that time was significant for TSH 2.41µIU/mL (0.35-4.94µIU/mL), Total T4 7.2ng/dL (4.9-11.7ng/dL), Free T4 1.28ng/dL (0.7 – 1.48ng/dL), WBC 3.8x103 µL-1, Hgb 13.5g/dL, platelets 95x103 µL-1. An electrocardiogram (ECG) showed nonspecific ST and T wave abnormalities. She underwent a nuclear stress test that was also unremarkable. By that time, she was placed on midodrine 5mg twice daily and presented again four months later complaining of varicose veins and leg edema. On that occasion, blood pressure had improved, midodrine was stopped, and she was started on furosemide 20mg daily as needed for edema. Four months later she presented once again with worsening edema, and furosemide dose was increased.
Concurrently, she underwent work-up for an ovarian cyst with high CA-125. As part of the work-up, abdominal and pelvic computed tomography (CT) incidentally demonstrated heterogeneous appearance of the liver and mild surface nodularity suggesting mild/early cirrhosis, mild-to slightly moderate ascites, and also moderate pericardial calcification extending from the base of the heart towards the apices of the ventricles, without pericardial effusion.
Further abdominal magnetic resonance imaging (MRI) characterized the cyst as a corpus luteum cyst. Esophagogastroduodenoscopy (EGD) revealed hypertensive gastropathy, non-bleeding erosive gastropathy, non-bleeding duodenal ulcers with clean base, and grade 1 esophageal varices. Comprehensive laboratory evaluation showed no evidence of underlying liver diseases such as viral or autoimmune hepatitis, hemochromatosis, Wilson's disease, primary biliary cirrhosis or primary biliary cholangitis.
At her current presentation, she denied fevers, chills, nausea, or abdominal pain. She also denied worsening of the edema.
Vitals: BP 129/83mmHg; HR 89bpm, RR 18bpm, Temp 36.2 C, SpO2 99% on room air.
On exam, she was dyspneic, though in no acute distress. Cardiac auscultation was significant for Kussmaul's sign and a pericardial knock.
Initial laboratory work-up showed CK 68U/L, MB 1%, Troponin T<0.01ng/mL, BNP 86pg/mL, INR 1.1, WBC 3.9x103 µL-1, Hgb 12.5g/dL, platelets 101x103 µL-1, BUN 15mg/dL, Cr 0.87mg/dL, K 3.8mEq/L, Na 141mEq/L, total bilirubin 0.7mg/dL, alkaline phosphatase 80U/L, ALT 21U/L, AST 20U/L, WSR 8mm/h, CRP 0.1mg/L.
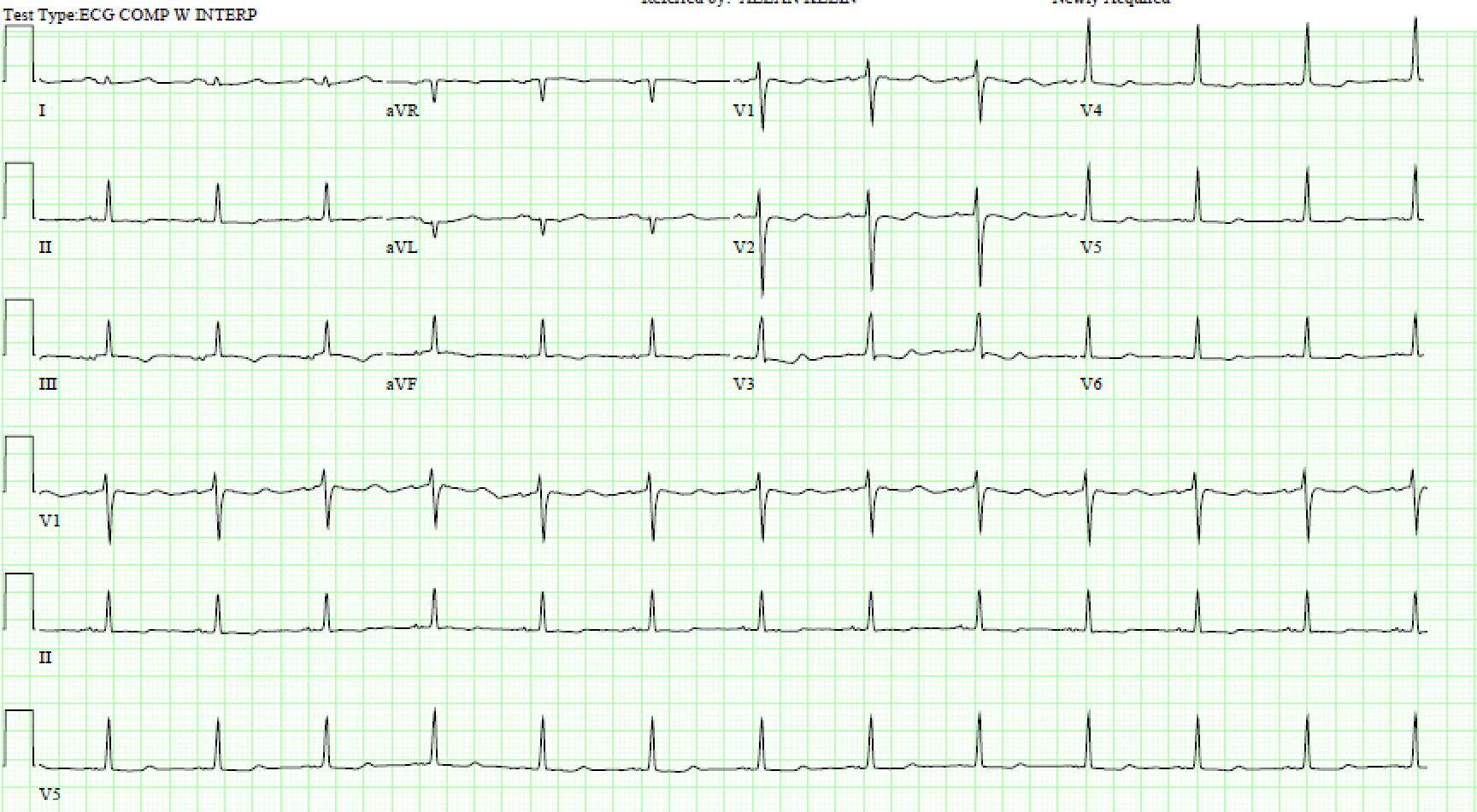
Electrocardiogram (ECG), additional imaging, and left and right heart catheterization were performed and are shown below (ECG 1 and Figure 1):
ECG 1
ECG 1
Figure 1
Figure 1
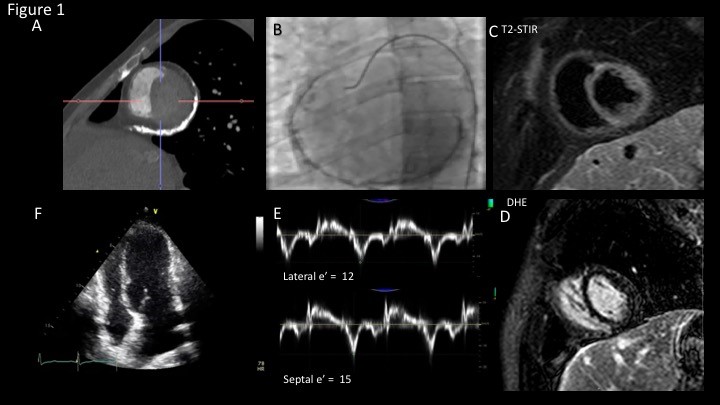
Figure 1: (A) Double oblique short axis orientation on cardiac CT demonstrating significant calcium burden along the lateral atrioventricular groove. (B) Circumferential pericardial calcification demonstrated on fluoroscopy (C) Short axis view on T2 short tau inversion recovery cardiac MRI sequence showing no pericardial enhancement. (D) Short axis view on delayed hyper enhancement sequences showing no increased pericardial signal to suggest pericardial inflammation (E) Tissue Doppler velocities of the septal and lateral mitral annulus. Doppler velocity with a compensatory increase in medial annular tissue Doppler velocity commonly referred to as "annulus reversus" (F) Apical 4 chamber window on transthoracic echocardiogram demonstrating conical/tubular deformity of the ventricles, suggestive of constrictive physiology.
Figure 1: (A) Double oblique short axis orientation on cardiac CT demonstrating significant calcium burden along the lateral atrioventricular groove. (B) Circumferential pericardial calcification demonstrated on fluoroscopy (C) Short axis view on T2 short tau inversion recovery cardiac MRI sequence showing no pericardial enhancement. (D) Short axis view on delayed hyper enhancement sequences showing no increased pericardial signal to suggest pericardial inflammation (E) Tissue Doppler velocities of the septal and lateral mitral annulus. Doppler velocity with a compensatory increase in medial annular tissue Doppler velocity commonly referred to as "annulus reversus" (F) Apical 4 chamber window on transthoracic echocardiogram demonstrating conical/tubular deformity of the ventricles, suggestive of constrictive physiology.
Left Heart Catheterization
Left Main Coronary artery
No disease
Left Anterior Descending Artery
No disease
Left Circumflex Artery
No disease
Right Coronary Artery
Dominant, tortuous, with no disease.
Right Heart Catheterization
Right Atrium
20mmHg (with deep y descent)
Right Ventricle
44/7mmHg
Pulmonary Artery
40/20mmHg (29 mmHg)
PCWP
22mmHg
Cardiac output
7L/min
Cardiac index
3.6L/min/m2
Simultaneous LV/RV pressure measurements revealed ventricular interdependence, with a systolic area index of 1.3, and presence of a square root sign.
What is the most appropriate next step in management?
Show Answer
The correct answer is: E. Refer for pericardiectomy
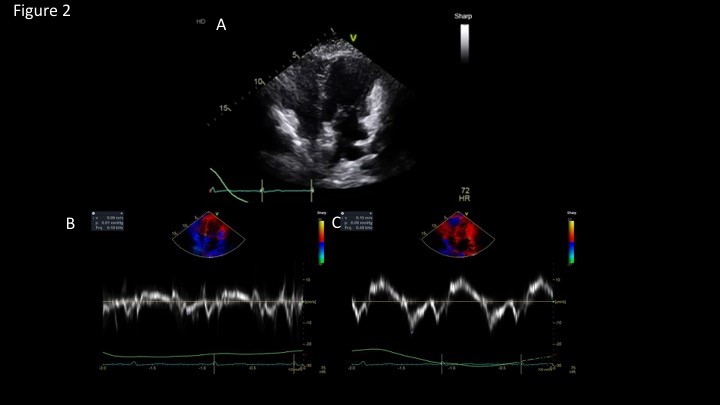
Overall, imaging findings are consistent with calcific constrictive pericarditis with no active inflammation of the pericardium (Figures 1 and 2).
Figure 2
Figure 2
Figure 2: Post pericardiectomy (A) Apical 4 chamber window on transthoracic echocardiogram demonstrating normal expansion of ventricles in end diastole. Normalization of the lateral (B) and septal (C) tissue Doppler velocities.
Figure 2: Post pericardiectomy (A) Apical 4 chamber window on transthoracic echocardiogram demonstrating normal expansion of ventricles in end diastole. Normalization of the lateral (B) and septal (C) tissue Doppler velocities.
Discussion
This patient's clinical history, features and imaging findings are consistent with chronic constrictive pericarditis. Constrictive pericarditis manifests as impaired diastolic filling of the ventricles.1 In constrictive pericarditis, symptoms are often insidious, with progressive signs and symptoms of right-sided heart failure, such as fatigue, peripheral edema and dyspnea, as the patient above. The most common reported causes are idiopathic/viral (42 – 49%), post-cardiac surgery (11-37%), post-radiation (9-31%), connective tissue disorder (3-7%), post-infectious (3-6%, either tuberculosis or purulent pericarditis), and miscellaneous causes (10%), such as malignancy, trauma, drug-induced, asbestosis, sarcoidosis and uremic pericarditis.1
A diagnostic suspicion of constrictive pericarditis is usually raised by symptoms and signs of right heart failure, with or without accompanying history of an inciting pericardial disease. Physical exam findings can include Kussmaul's sign, which is the failure of an appropriate fall or paradoxical rise in jugular venous pressure (JVP) during inspiration. This happens due to high pressures in an encased right atrium, that are resistant to the flow through the superior vena cava during inspiration. The "pericardial knock" is the high-pitched sound audible in early diastole from sudden cessation of rapid ventricular filling.1,2
Multiple diagnostic tools can aid in defining constrictive pericarditis, although clinical suspicion is always paramount. ECG can show low voltages, non-specific ST/T changes (as in this patient case), or atrial fibrillation. Chest X-ray can show pericardial calcifications in one-third of the cases.1 CT and MRI have an important role. Pericardial thickness > 3-4mm can be seen on both. On CT, pericardial calcifications can be also seen, given that this modality is the most accurate imaging technique to identify calcified tissue.1 Furthermore, although the diagnosis of constrictive pericarditis can often be made with a thorough history, physical exam and a chest X-ray, identifying active inflammation and/or a potentially reversible cause of constrictive pericarditis requires pericardial characterization by cardiovascular magnetic resonance (CMR). On CMR, specifically using dark blood, bright blood cines, T2STIR (edema) based sequence, and delayed hyper-enhancement sequences, we can identify a thickened pericardium, features of constrictive physiology, pericardial edema and pericardial inflammation respectively.3 Ventricular interdependence may be observed with real-time cine imaging.1,3
The presence of calcium on imaging suggests a chronic calcific pericardial process, though excluding inflammation is important and can, in some cases, save the patient a pericardiectomy in the setting of "transient constrictive pericarditis". Further, absence of inflammation during a pericardiectomy has important surgical/technical implications, with less inflammation being more favorable at the time of surgery.4
Although not always required, left and right cardiac catheterization remains the gold standard to evaluate for the presence and hemodynamic significance of constriction, and also to differentiate constrictive to restrictive heart disease in circumstances of uncertain diagnosis (e.g. radiation heart disease). It is indicated (Class I-C) when non-invasive diagnostic methods do not provide definite diagnosis of constriction.1 In cardiac catheterization, constrictive physiology will show an equalization of right and left cardiac pressures, a rapid "y" descent on atrial pressure waveforms, and a "square root" or "dip and plateau" sign on ventricular pressure waveforms. Ventricular diastolic pressures are high but stroke volume is low because of insufficient pre-load.1,2,5 Additionally, there is isolation of the cardiac chambers from variations in intra-thoracic pressures during the respiratory cycle. Ventricular interdependence is assessed by systolic area index, which is the change in the ventricular pressure area between inspiration and expiration. A systolic area index above 1.1 has been shown to be predictive of constrictive pericarditis, with 97% sensitivity and 100% specificity in surgically proven patients.1,5
The recommended treatment for chronic permanent constriction is complete surgical resection of the pericardium (radical pericardiectomy). In some cases, if there is evidence of extensive pericardial inflammation and suggestion of a more early/acute phase of the illness, a trial of anti-inflammatory therapy and symptom management may be reasonable, with assessment for reversibility within three months.4,6,7 This may preclude the need for surgery, or reduce the technical difficulty of future surgery by resolving underlying inflammation.
Medical therapy may have a role in at least three conditions:
Treat underlying etiology if reversible (i.e. tuberculosis, to reduce risk of progression to constriction)
Treat underlying inflammation to resolve transient constriction (as evidenced by elevated inflammatory markers and imaging findings) – treatments include colchicine, NSAIDS, prednisone, etc.1,6,7
Symptomatic management of right heart failure (i.e. diuretics)
It is important to keep in mind that, if pericardiectomy is possible, medical therapy should not delay the procedure, unless surgery is high risk or contraindicated.
Based on this case, the patient appears to have developed chronic constrictive pericarditis over time, possibly since her first presentation for palpitations, hypotension and edema, two years before referral to pericardiectomy. Furthermore, supporting imaging findings of a significant calcium burden (CT and chest X-ray, constrictive physiology by echo, MRI and catheterization, with negative inflammatory biomarkers (CRP and WSR) along with no signs of pericardial inflammation on CMR suggested a more chronic course. Most importantly, right heart failure resulting in underlying cirrhosis, with established portal hypertension and thrombocytopenia, meant that referral for pericardiectomy was the most appropriate course of management before she developed more significant liver dysfunction, which would have precluded surgery. She underwent successful pericardiectomy two months after presentation and continued to do well after surgery, completing cardiac rehabilitation. Diuretics were progressively tapered off and her platelet count stabilized. She continues to do well months after the procedure.
References
Adler Y, Charron P, Imazio M, et al. The 2015 ESC guidelines on the diagnosis and management of pericardial diseases. Eur Heart J 2015;36:2921-64.
Geske JB, Anavekar NS, Nishimura RA, Oh JK, Gersh BJ. Differentiation of constriction and restriction: complex cardiovascular hemodynamics. J Am Coll Cardiol 2016;68:2329-47.
Chetrit M, Xu B, Kwon DH, et al. Imaging-guided therapies for pericardial diseases. JACC Cardiovasc Imaging 2019. [Epub ahead of print].
Unai S, Johnston DR. Radical pericardiectomy for pericardial diseases. Curr Cardiol Rep 2019;21:6.
Talreja DR, Nishimura RA, Oh JK, Holmes DR. Constrictive pericarditis in the modern era: novel criteria for diagnosis in the cardiac catheterization laboratory. J Am Coll Cardiol 2008;51:315-9.
Haley JH, Tajik AJ, Danielson GK, Schaff HV, Mulvagh SL, Oh JK. Transient constrictive pericarditis: causes and natural history. J Am Coll Cardiol 2004;43:271-5.
Cremer PC, Kumar A, Kontzias A, et al. Complicated pericarditis: understanding risk factors and pathophysiology to inform imaging and treatment. J Am Coll Cardiol 2016;68:2311-28.