A 66-year-old Caucasian female patient was admitted to the emergency room with complaints of shortness of breath, pleuritic chest pain and cough that appeared two days earlier. Two weeks earlier she suffered symptoms of an upper respiratory tract infection. Her medical history was unrevealing. Physical examination on admission revealed shortness of breath. Her pulse was 80 bpm, her blood pressure was 120/60 mmHg, her body temperature was 37 degrees Celsius. Her heart sounds were muffled, her neck veins were not distended. Her lung fields were clear except for decreased breathing sounds on the left base without crepitations or wheezing. Her electrocardiogram showed sinus tachycardia with diffuse ST segment elevation. Laboratory examination revealed hs-C-reactive protein level of 24.3 mg/dl. glucose 106 mg/dl, creatinine 0.48 mg/dl, urea 26 mg/dl, sodium 133 mg/dl, cardiac troponin T level was <0.01 ng/dl (normal range, 0.0-0.1 ng/dl) white blood cell count was 11,420 cells/mcl with 74.5% neutrophils.
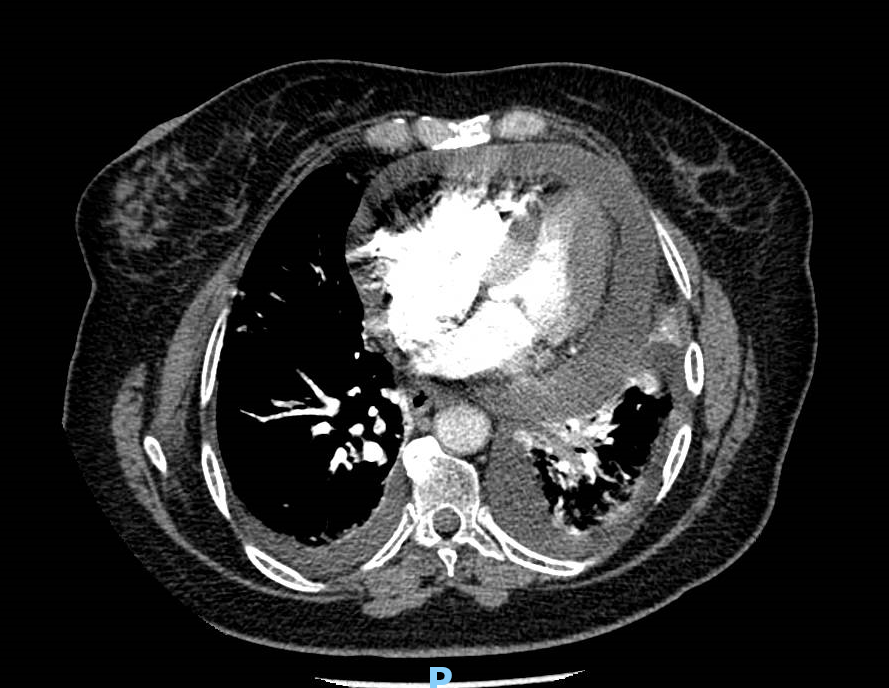
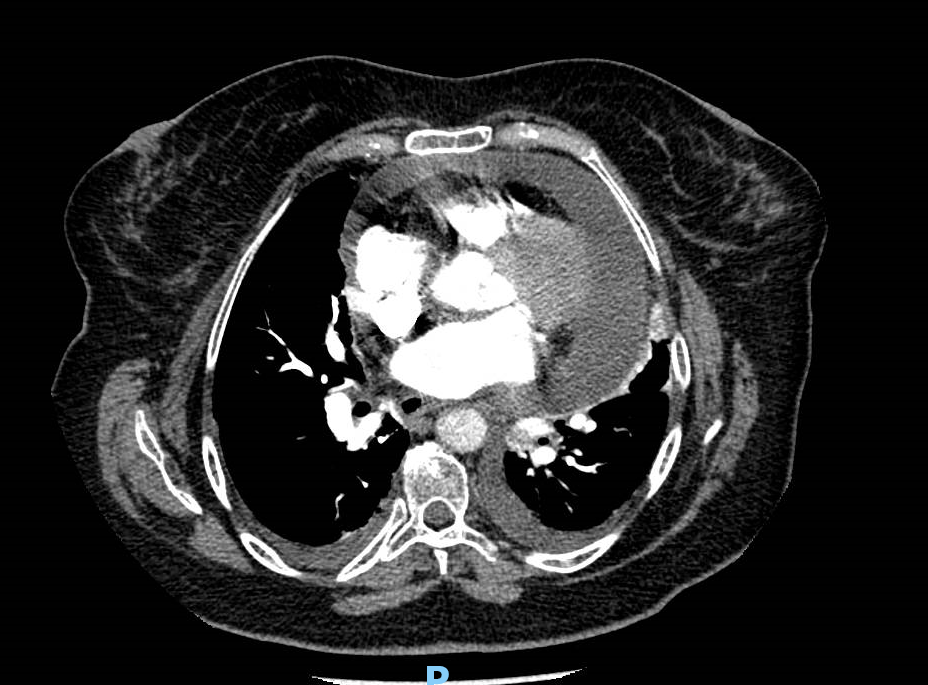
She underwent emergent computerized chest tomography (CT) (Figures 1-3).
Figure 1
Figure 1
Figure 2
Figure 2
Figure 3
Figure 3
Which of the following best describes the CT findings?
Show Answer
The correct answer is: D. A large pericardial effusion with small bilateral pleural effusion
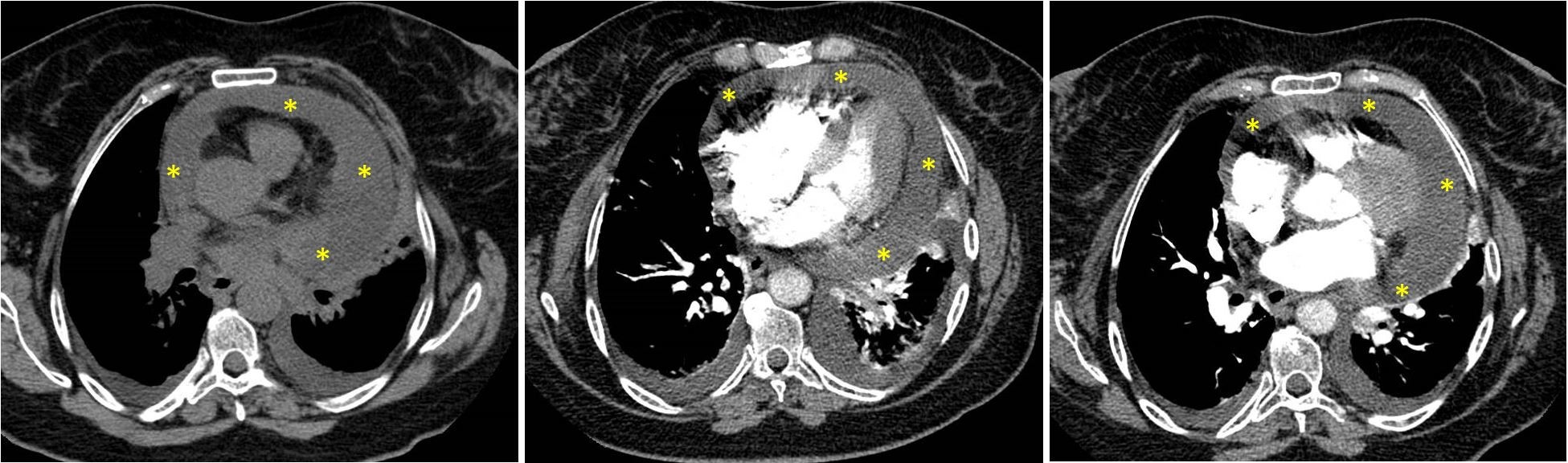
The CT revealed a large pericardial effusion and small bilateral pleural effusion (pericardial effusion indicated by yellow asterisk on Figure 4). No evidence for pulmonary embolism or pneumonia were found.
Figure 4
Figure 4
Shortly afterwards, the patient's blood pressure decreased. An emergent echocardiogram revealed a large pericardial effusion with respiratory flow variation >25% across the mitral valve, diastolic collapse of the right atrium, and early diastolic collapse of the right ventricular free wall. The patient underwent emergent pericardiocentesis with prompt relief of her symptoms. Treatment with ibuprofen 800 mg TID and colchicine 0.5 mg BID was started. The rest of her hospital course was uneventful, and she was discharged 3 days later.
Discussion
The patient presented with shortness of breath and pleuritic chest pain that appeared 2 weeks after an upper respiratory tract infection.
The differential diagnosis of pleuritic chest pain includes mainly acute pericarditis, pleuropneumonia, acute pulmonary embolism, and musculoskeletal pain.
Diffuse ST segment elevation is a typical hallmark sign of acute pericarditis, reported in up to 60% of the patients.1 ST segment elevation can occur in pulmonary embolism and can be a poor prognostic sign. However, ST segment elevation in pulmonary embolism are not described as diffuse, and other signs, for example S1Q3T3 pattern, right axis deviation, p pulmonale and right bundle branch block are more typical.2 A viral prodrome is reported in >50% of the patients with acute idiopathic pericarditis.3 Upper respiratory tract infection often precedes acute idiopathic pericarditis and can support the diagnosis of acute pericarditis in the patient. A markedly elevated hs-CRP level is sensitive but not specific to acute inflammation. However, in acute pericarditis, increase in hs-CRP level is very common and markedly elevated levels are associated with major cardiac complications.3 Therefore, if the patient had acute pericarditis, a large pericardial effusion with risk of cardiac tamponade is more likely than a small or no effusion. Moreover, hs-CRP levels in acute pericarditis correlate with pleural effusion.4 Pleuropneumonia and skeletal pain can lead to shortness of breath and pleuritic chest pain, but ST segment elevation is unlikely in these cases. The patient had no history of chest trauma and there were no findings on physical examination suggestive of a rib fracture. In addition, markedly elevated hs-CRP level is unlikely in this case.
The chest CT confirmed the presence of pericardial effusion and ruled out pulmonary embolism and pleuropneumonia. The diagnosis of acute idiopathic pericarditis is clinical. Current guidelines recommend that the diagnosis should be considered on presence of at least two of the following criteria: typical pleuritic chest pain, typical electrocardiographic changes, new or worsening pericardial effusion, and pericardial friction rub.1 As the patient had pericardial effusion, typical chest pain and diffuse ST segment elevation, three of the diagnostic criteria of acute pericarditis were met.1 In acute pericarditis, high-sensitivity C-reactive protein becomes elevated in 97.8% of the patients.3 It rises rapidly and becomes elevated in 92.3% of the patients within 12 hours of onset of symptoms.3 Thus, it can be helpful in the early diagnosis of acute pericarditis. Maximal hs-CRP level in acute pericarditis is associated with frequency of major cardiac events, including cardiac tamponade, and thus has prognostic significance.3 The patient presented here had a large pericardial effusion and cardiac tamponade, as could be expected in view of her markedly elevated high-sensitivity C-reactive protein level. Shortness of breath is not typical to acute pericarditis but has been found in a minority of the patients with acute pericarditis. Dyspnea can appear in patients with acute pericarditis, presumably when pleuritic pain limits breathing, when there is a concomitant large pleural effusion, or when cardiac tamponade is accompanied by peripheral hypoperfusion and acidosis. A relationship has also been described between the size of pericardial effusion and dyspnea.5
References
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Digby GC, Kukla P, Zhan ZQ, et al. The value of electrocardiographic abnormalities in the prognosis of pulmonary embolism: a consensus paper. Ann Noninvasive Electrocardiol 2015;20:207-23.
Mager A, Hammer Y, Ofek H, Kedmi I, Iakobishvili Z, Kornowski R. Prognostic and diagnostic significance of serum high-sensitivity C-reactive protein level in patients with acute idiopathic pericarditis. Isr Med Assoc J 2019;21:747-51.
Lazaros G, Antonopoulos AS, Imazio M, et al. Clinical significance of pleural effusions and association with outcome in patients hospitalized with a first episode of acute pericarditis. Intern Emerg Med 2019;14:745-51.
Mager A, Birnbaum Y, Adler Y, Imbar S, Strasberg B, Battler A. The anteroposterior pericardial sac diameter measured by echocardiography correlates with the volume of pericardial effusion and with effort dyspnea. Eur J Echocardiogr 2005;6:358-62.