Can I Have Constrictive Pericarditis Six Years After Transient Constriction?
A 57-year-old female with a history of viral pericarditis, hypothyroidism, and atrial flutter status post direct current electrical cardioversion presents to the office with a chief complaint of dyspnea. She was diagnosed with viral pericarditis 30 years prior to her current presentation, and then 6 years prior to presentation, she developed constrictive pericarditis which has been managed conservatively with furosemide 20 mg daily and spironolactone 25 mg daily. Since her symptoms have stabilized, surgery was not indicated. Over the past 3 months, she has developed worsening dyspnea with minimal exertion, to the point that she can no longer put on her shoes without losing her breath.
On examination, she was afebrile, heart rate was 109 beats per minute and irregular, blood pressure was 116/75 mmHg, and her SpO2 on room air was 96%. She had jugular venous distension to the angle of her jaw while lying at 45 degrees, a positive Kussmaul's sign, a pericardial knock, and 2+ pitting edema in her bilateral lower extremities.
Echocardiography revealed inspiratory ventricular septal interdependence towards the right ventricle (Clip), and an increased septal (Figure 1A) and lateral (Figure 1B) mitral annular velocity on tissue Doppler. Left heart catheterization did not show obstructive coronary disease. To better visualize calcified pericardium, cardiac computed tomography was done and showed severe nodular calcification of the pericardium with posterior mitral annular calcifications (Figure 2).
Clip: Apical four chamber view of transthoracic echocardiography showing inspiratory ventricular septal interdependence towards the right ventricle
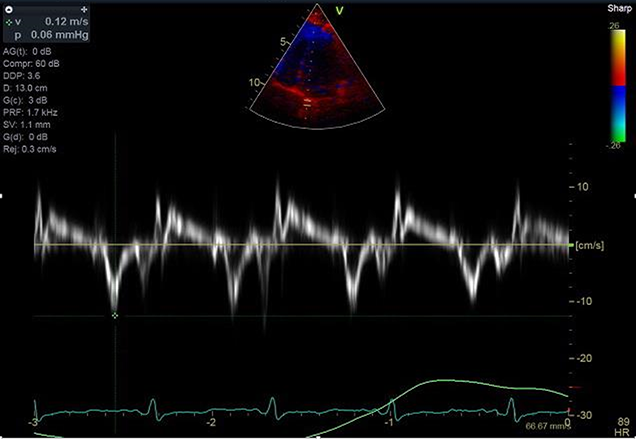
Figure 1(A-B): Doppler echocardiography showing increased septal early diastolic mitral annular velocity (0.12m/s) (A) compared to lateral early diastolic mitral annular velocity (0.8m/s) (B)
(A)
(B)
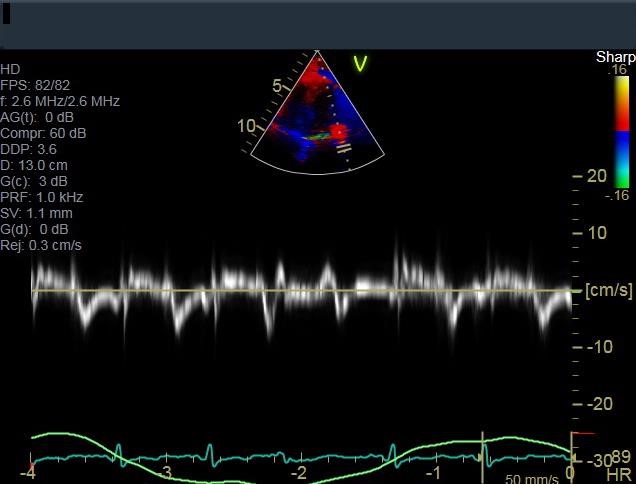
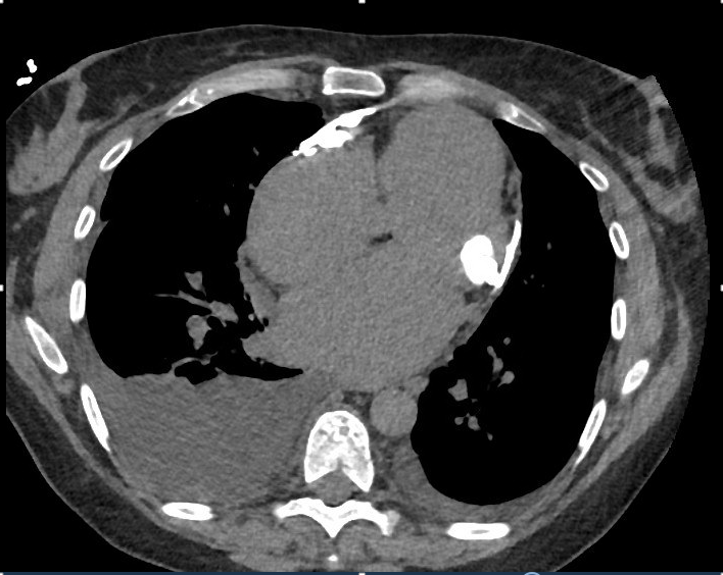
Figure 2: Chest computed tomography showing severe calcifications of the pericardium, posterior mitral annular calcifications, and moderate right pleural effusion
Which of the following invasive hemodynamic findings is most consistent with a diagnosis of constrictive pericarditis?
Show Answer