A 76-year-old gentleman with a past medical history of coronary artery disease (CAD), diabetes, atrial fibrillation, and hypertension is admitted to the hospital for management of severe three-vessel CAD. Prior to admission, he developed unstable angina, which was evaluated by a nuclear stress test which was markedly positive. He was referred for left heart catheterization, which revealed three-vessel disease with a 99% stenosis in the distal left main artery, a 95% proximal stenosis in the proximal left anterior descending artery, an 80% stenosis in the ostial circumflex, and a 70% lesion in the proximal right coronary artery.
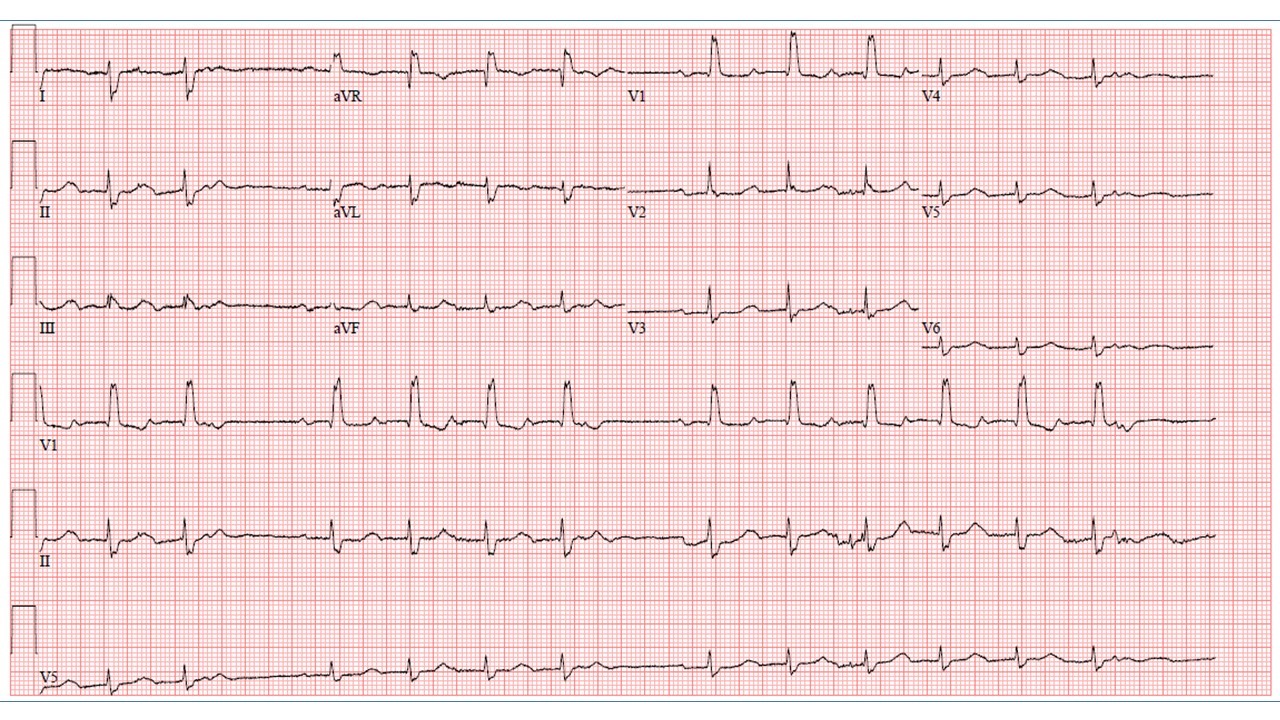
Figure 1
An ECG performed upon admission demonstrates which of the following:
Show Answer
The correct answer is: C. Sinus rhythm with premature complexes
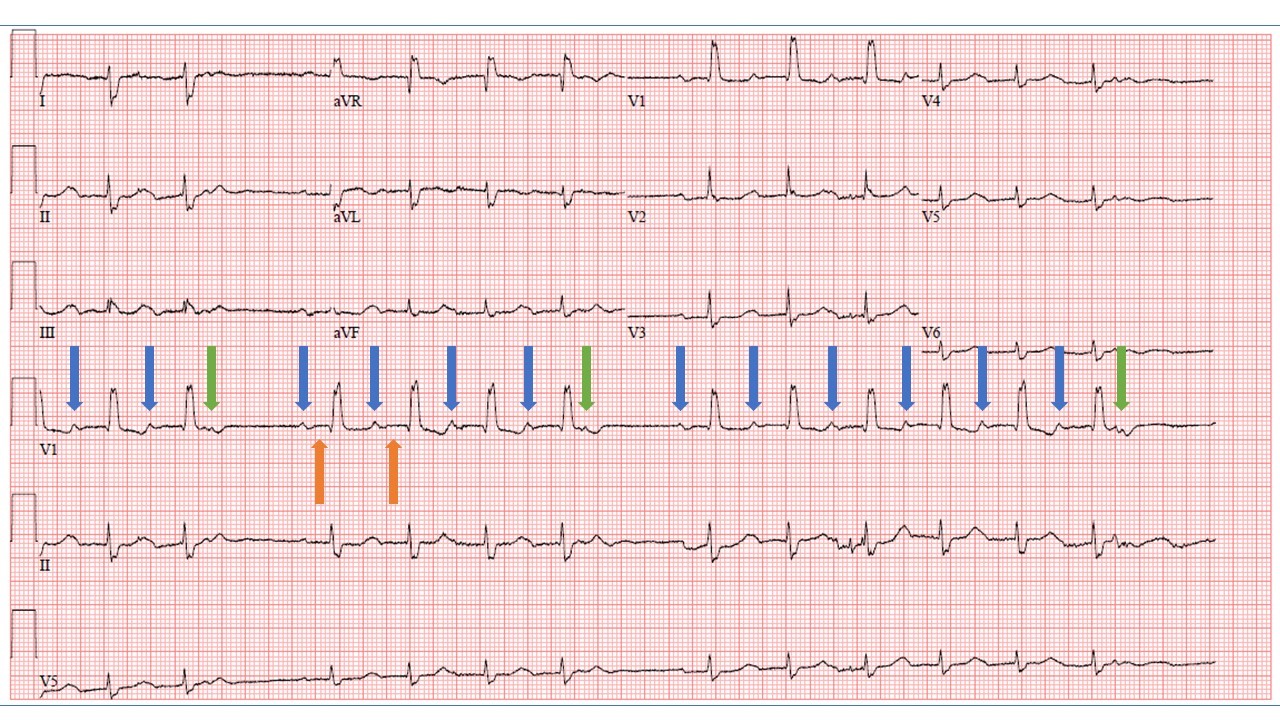
This ECG demonstrates sinus rhythm with a first-degree AV block, atrial premature contractions (APCs), premature atrial contractions, and compensatory pauses. Sinus P waves are present throughout the tracing (blue arrows) and clearly precede each QRS complex. An APC can be seen "buried" within the third and seventh T waves (green arrow), most easily appreciated in lead V1. However, this APC is not conducted to the ventricles since it reaches the AV node during its absolute refractory period. The next sinus P wave is delayed, as it follows a compensatory pause. Following the pause, the first PR interval is shorter than the second PR interval (orange arrows) due to decremental conduction of the AV node.1
Since the PR intervals do not consistently prolong prior to dropped beats, answer A is incorrect. Second degree AV block (choices A and B) are not correct because, while there may appear to be group beating with dropped QRS complexes, the beats are not consistently grouped, and the P waves are not conducting regularly (indeed, the non-conducted atrial beat comes early). This is not atrial fibrillation (Choice D) because atrial activity is present.
Figure 2
References
Watanabe Y, Watanabe M. Impulse formation and conduction of excitation in the atrioventricular node. J Cardiovasc Electrophysiol 1994;5:517-31.