Acute severe mitral regurgitation will result in hemodynamic instability requiring rapid intervention.
It is important to determine the etiology of mitral regurgitation to guide medical management. Identifying the infectious responsible agent, if present, is essential to determine appropriate long-term therapy after surgery.
A previously healthy 13-month-old male presented to the Emergency Department with 7 days of cough, congestion and intermittent fever to a maximum of 104.8F, decreased oral intake and new increased work of breathing. On exam, there was a grade 2-3/6 holosystolic murmur at the left lower sternal border, intermittent S3 gallop and hepatomegaly to 3 cm below the right costal margin. He was initially diagnosed with pneumonia and was given empiric antibiotics and a fluid bolus. He failed to respond to non-invasive respiratory support, became hypotensive and required rapid-sequence intubation with pressor support. Troponin and b-type natriuretic protein levels were elevated at 0.15 ng/mL (reference range for normal < 0.03) and 995.5 pg/mL (reference range <100), respectively. A chest x-ray (Figure 1), electrocardiogram (Figure 2) and transesophageal echocardiogram (Figure 3) are shown below.
Figure 1
Figure 1
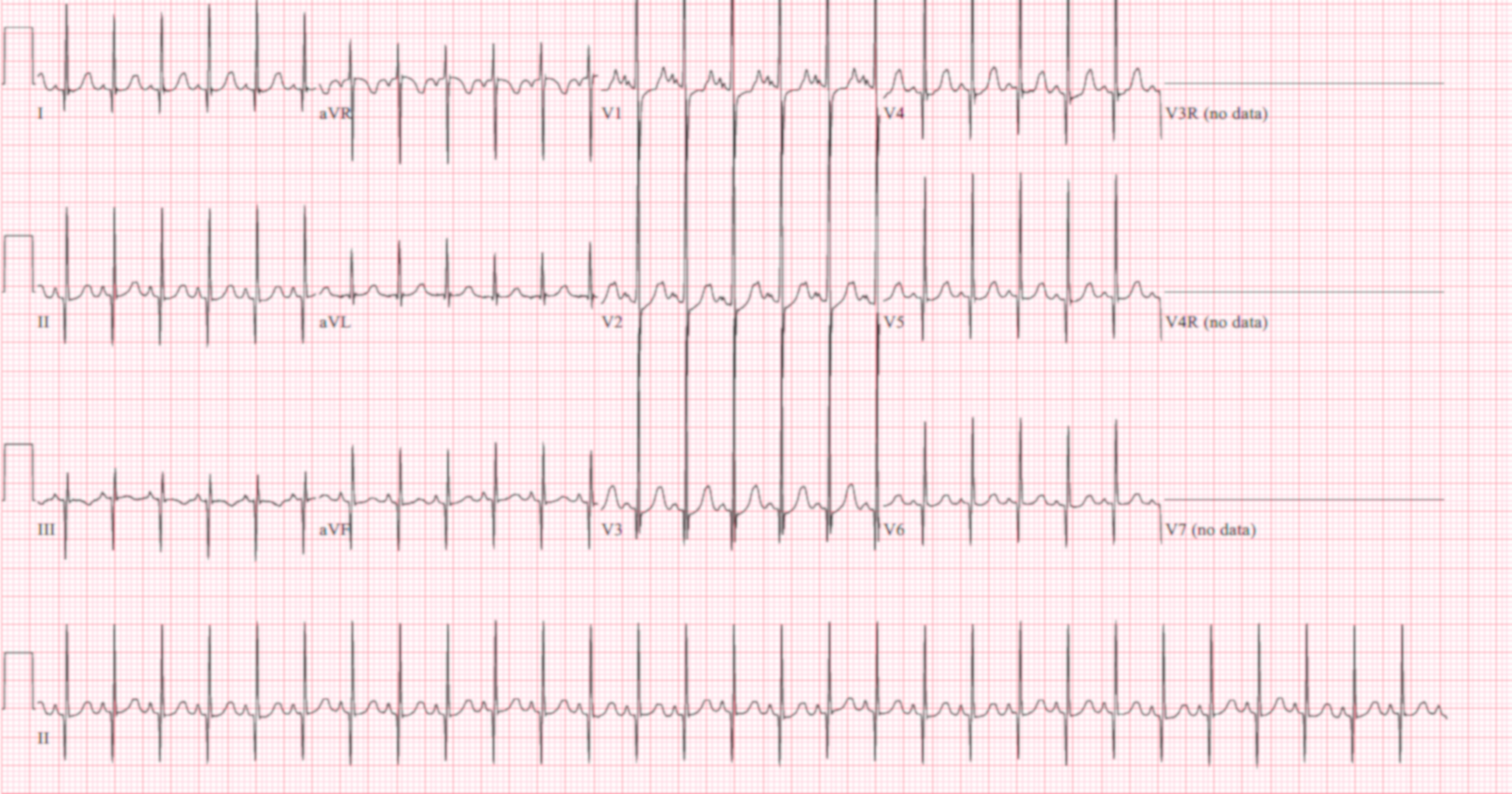
Figure 2
Figure 2
Figure 3
Figure 3
What is the most likely cause of the patient's clinical deterioration?
Show Answer
The correct answer is: C. Endocarditis with a vegetation in the mitral chordae and subsequent chordal erosion.
Figure 1, the chest x-ray upon presentation, shows multifocal pulmonary opacities and a small right pleural effusion, with a normal cardiac silhouette. Figure 2, the electrocardiogram on admission, shows sinus tachycardia, right ventricular hypertrophy with possible biventricular hypertrophy and nonspecific ST and T wave abnormalities. Figure 3, a color-compare 4-chamber transesophageal echocardiogram shows a flail posterior leaflet and severe mitral regurgitation originating from an area of poor leaflet coaptation. There is a finger-like mobile echo-density adherent to the chordal attachments of the posterior mitral valve leaflet. These findings make choice C the most likely diagnosis.
The severity of mitral regurgitation and the child's rapid clinical deterioration required prompt intervention.1 Intraoperative findings confirmed the presence of vegetations along the chordal attachments of the posteromedial papillary muscle, causing erosion of the chordae and subsequent flailing of P2 and P3 of the posterior mitral valve leaflet. He underwent mitral valve repair with chordal resuspension, commissuroplasty and annuloplasty as well as removal of the vegetation from the posteromedial papillary muscle. His blood cultures grew Kingella kingae (an HACEK organism). He recovered from the operation uneventfully and completed 6 weeks of IV ceftriaxone. He is now doing well at home, with mild mitral regurgitation.
A is incorrect. In infants, ischemia causing papillary muscle rupture can occur in the setting of anomalous left coronary artery arising from the pulmonary artery (ALCAPA), but the timing of presentation would be at a much younger age than this patient.2 This child was previously well, with no concerns in his history that might allude to this diagnosis. Furthermore, the left ventricle (LV) systolic function was normal by echo, making this diagnosis unlikely.
B is incorrect. Long-standing severe mitral regurgitation would have resulted in left heart dilation, which is not present in the case. The clinical presentation suggests an acute or sub-acute infectious disease process. Furthermore, the mitral valve anatomy in this patient argues against a congenital mitral valve anomaly.3
D is incorrect. The mitral annulus and LV are not dilated in this patient, nor is there LV systolic dysfunction, making cardiomyopathy unlikely.4
E is incorrect. While chordal rupture can rarely be seen with acute rheumatic heart disease, the age of the patient makes acute rheumatic fever less likely. The incidence of acute rheumatic fever is highest in children between the ages of 5 and 15 years. In the United States, acute rheumatic fever is very rare in children 3 years of age and younger. Additionally, the classic findings of rheumatic valvulitis, such as shortened chordal attachments and diffusely thickened leaflets, are not present.5
References
Baltimore RS, Gewitz M, Baddour LM, et al. Infective endocarditis in childhood: 2015 update – a scientific statement from the American Heart Association. Circulation 2015;132:1487-1515.
Patel SG, Frommelt MA, Frommelt PC, Kutty S, Cramer JW. Echocardiographic diagnosis, surgical treatment, and outcomes of anomalous left coronary artery from the pulmonary artery. J Am Soc Echocardiogr 2017;30: 896-903.
Moss AJ, Allen HD. "Anatomic and Functional Mitral Valve Abnormalities in the Pediatric Population." In: Moss and Adams' Heart Disease in Infants, Children and Adolescents: Including the Fetus and Young Adult. 9th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins;2016.