A 63-year-old female with a past medical history of non-alcoholic steatohepatitis, cirrhosis, refractory ascites, encephalopathy, gastrointestinal bleeding, type II diabetes, heart failure with preserved ejection fraction, obstructive sleep apnea, and paroxysmal atrial fibrillationpresents to the emergency department (ED) with immense fatigue and weakness.
Figure 1
Figure 1
Her continuous cardiac monitoring in the ED demonstrates which of the following:
Show Answer
The correct answer is: D. Sinus bradycardia with junctional escape beats.
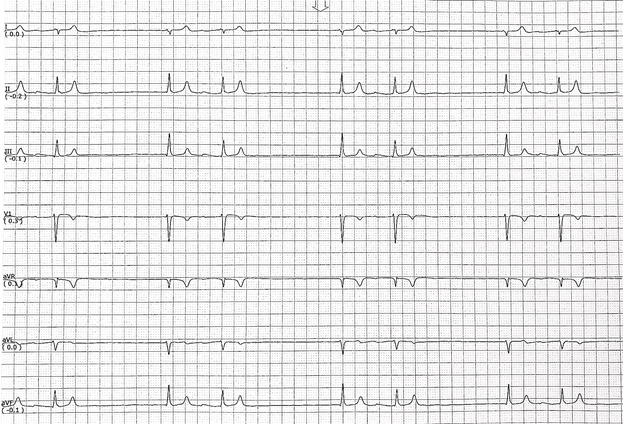
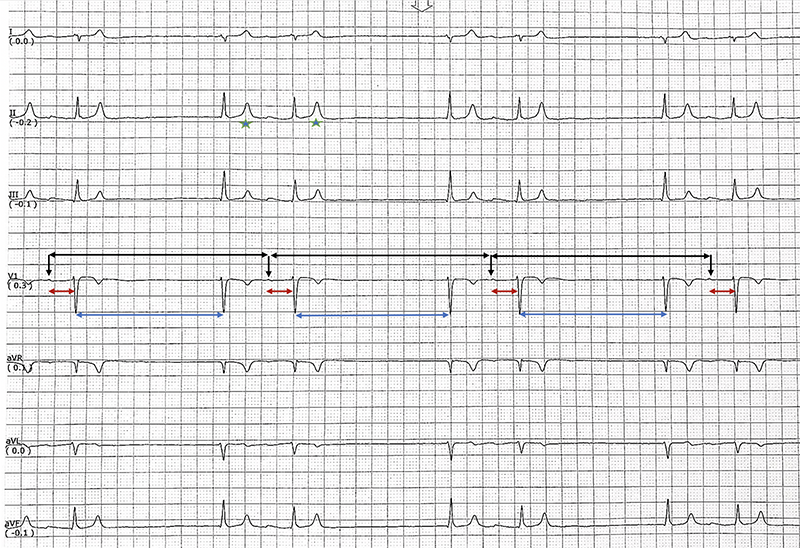
The first beat of the rhythm strip is sinus beat with a significant reduction of P wave amplitude (Figure 2 - black arrow) as well as prolongation of the PR interval to 300 ms (Figure 2 - red double-sided arrow). The second beat is a junctional escape beat with an interval length of 1860 ms corresponding to a heart rate of 32 bpm. The third beat is another sinus beat with the same characteristics of the first beat. The interval between the first and third sinus beats is 2760 ms corresponding to severe sinus bradycardia with a heart rate of 22 bpm (Figure 2 - black double-sided arrow). The fourth beat is another junctional beat with same coupling interval from sinus beat (Figure 2 - blue double-sided arrow). This pattern is repeated periodically, which creates an irregularly regular rhythm. Therefore, answer A, atrial fibrillation, is not the correct answer.
There is no P wave before the second, fourth, and sixth beats; therefore, answer B, sinus bradycardia with atrial bigeminy, is incorrect.
There is no blocked P wave; therefore, answer C, sinus bradycardia with second-degree AV block type II is incorrect.
The T wave is peaked with a narrow base in lead II (Figure 2 - green stars).
Figure 2
Figure 2
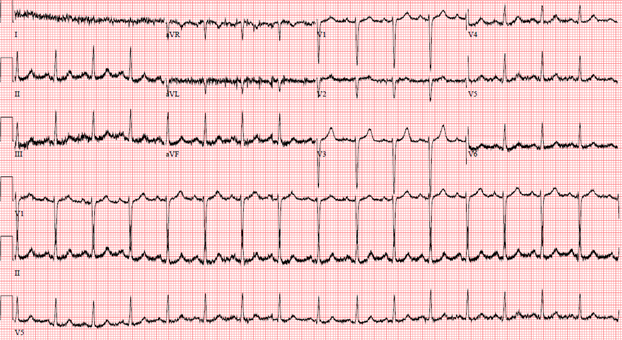
All of the above changes are related to moderate hyperkalemia. The serum potassium in this patient was 7.5 mEq/L. Appropriate emergent treatment restored normal sinus rhythm (Figure 3) with normal serum potassium level at 4.5 mEq/L.
Figure 3
Figure 3
Mattu and colleagues reported all ECG and rhythm changes corresponding to different level of hyperkalemia.1
Mild hyperkalemia 5.5-6.5 mEq/L:
Tall, tent-shaped ("peaked") T-waves with narrow base, best seen in precordial leads