A 57-year-old female with a history of idiopathic ventricular tachycardia status post dual-chamber implantable cardioverter-defibrillator (ICD), paroxysmal atrial fibrillation, and hypothyroidism presents to her local emergency department with a chief complaint of dyspnea. The patient's recent medical history is notable for an ICD lead extraction 3 weeks prior to her current presentation that was complicated by superior vena cava (SVC) laceration. The procedure required emergent sternotomy for pericardial hematoma evacuation and repair of the SVC laceration via a bovine pericardial patch repair. Since discharge, she has noted progressively worsening dyspnea and fatigue, and she presented to the emergency department after development of lightheadedness over the past 2 days.
On examination, she appeared distressed with vital signs noting afebrile temperature, heart rate 127 beats per minute and irregular, blood pressure 107/66 mmHg, respiratory rate 20, and oxygen saturation 99% by pulse oximetry on 2 liters of supplemental oxygen via nasal cannula. Heart sounds were distant on auscultation, and jugular venous distension was evident to the angle of the mandible sitting upright.
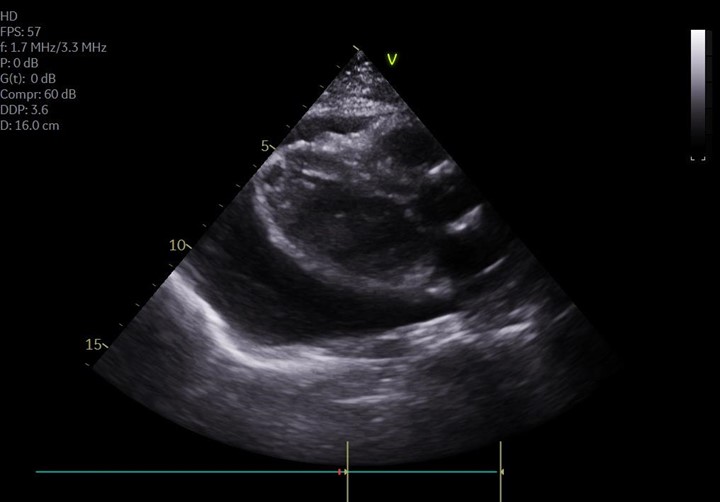
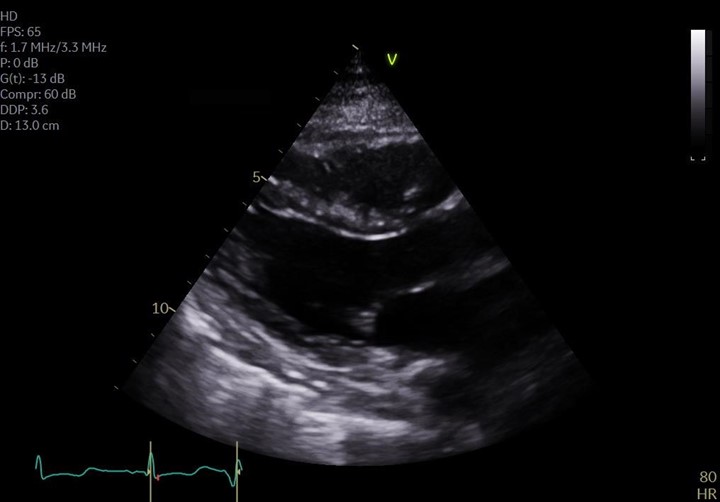
Electrocardiogram was notable for atrial fibrillation and low voltage across the precordium. Chest x-ray showed an enlarged cardiac silhouette. A limited point of care echocardiogram was notable for a very large pericardial effusion (Figure 1a). The patient underwent emergent pericardiocentesis via the apical approach with removal of 500 mL of pericardial fluid (Image 1). The patient had rapid improvement in symptoms and vital signs following drainage (Figure 1b).
Figure 1: Point of care echocardiogram with representative parasternal long axis images identifying a large pericardial effusion and tamponade physiology (a) and resolution of effusion following pericardiocentesis (b).
Figure 1a
Figure 1a
Figure 1b
Figure 1b
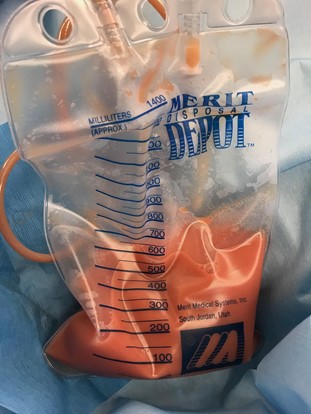
Image 1: Pericardial fluid following aspiration via pericardiocentesis.
Image 1
Pericardial fluid analysis is shown below (Table 1), which was notable for turbid fluid with elevated red blood cells, a lymphocytic predominance, and triglycerides with the presence of chylomicrons.
Table 1: Pericardial fluid analysis.
pH
Clarity
RBC
WBC
Lymph %
Protein
LDH
Gram stain
Cytology
Triglycerides
Chylomicrons
7.36
Turbid
34,000/uL
2,736/uL
88%
4.4 g/dL
390 U/L
Negative
Negative
663 mg/dL
Present
What is the etiology of this patient's pericardial effusion?
Show Answer
The correct answer is: B. Chylopericardium
The patient's pericardial fluid analysis confirms the diagnosis of chylopericardium. Chylopericardium is suspected with the aspiration of turbid pericardial fluid classically described as "milky" in appearance, with subsequent pericardial fluid analysis typically revealing an elevated triglyceride content >500 mg/dL, a cholesterol/triglyceride ratio <1.0, negative fluid cultures, and a lymphocytic predominance.1
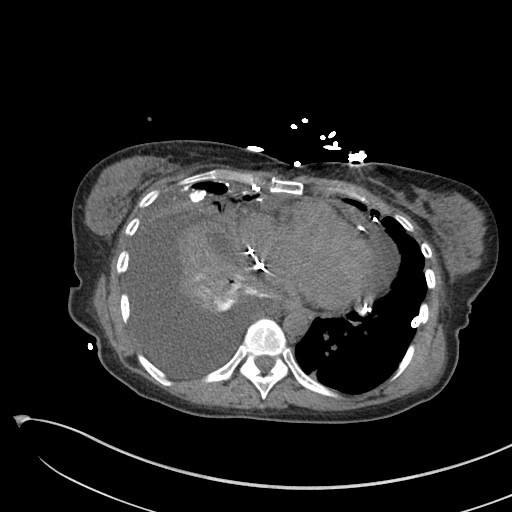
Chylous pericardial effusions are rare, and more commonly the effusion is secondary to trauma, surgical injury, or malignant obstruction of the thoracic duct.2 Primary idiopathic chylopericardium is an exceedingly rare diagnosis, with even contemporary reviews on the subject identifying just over 100 cases in the literature.3,4 Clinically, chylopericardium presents similarly to other etiologies of effusion, though on computed tomography (CT) imaging the chylous effusion can display attenuation less dense than water.2 A follow-up chest CT performed shows a residual pleural effusion with low attenuation fluid consistent with chylothorax (Figure 2).
Figure 2: Chest CT of the patient with a large right pleural effusion notable for low attenuation fluid, consistent with chylothorax.
Figure 2
Conservative management of chylopericardium is similar to that of chylothorax, with a modified diet that is low in dietary fat with medium-chain triglyceride (MCT) supplementation to mitigate generation of chyle.5,6 Conservative management was successful in 55% of previously published cases, which is similar to the approximately 50% success rate in the treatment of chylothorax.7 These patients sometimes require further dietary supplementation via total parenteral nutrition (TPN). Case reports have also evaluated the use of octreotide in chylothorax and chylopericardium, leading to decreased chyle production.8,9 For those patients that fail conservative management, current practice generally involves surgical ligation of the thoracic duct via open thoracotomy or video-assisted thoracoscopic surgery (VATS), often combined with partial pericardiectomy due to the risk of future constrictive pericarditis.1,7,10,11
The patient described in this case suffered iatrogenic laceration of her thoracic duct during the complicated ICD lead extraction and emergent repair of her SVC injury. The chylous fluid shown here has a notable reddish tint, likely from the introduction of blood in the perioperative period, rather than a classic milky white appearance. She underwent emergent pericardiocentesis as described above for the development of tamponade physiology and was subsequently started on conservative therapy with a low fat diet, medium-chain triglyceride supplementation, and TPN. She was unable to tolerate MCT supplementation and was discharged on dietary modification and TPN. Unfortunately, the patient had early recurrence of chylopericardium with tamponade and required repeat pericardiocentesis with subsequent temporizing pericardial window. Later evaluation by lymphangiography did not clearly identify a thoracic duct despite evidence of extravasated lipiodol around the heart and right pleural space. During subsequent intervention via VATS, the thoracic duct was not amenable to ligation due to adhesions, so the patient underwent mechanical and doxycycline pleurodesis. She has since gradually reintroduced a normal diet without recurrence of chylopericardium or chylothorax.
References
Dib C, Tajik AJ, Park S, Kheir MEL, Khandieria B, Mookadam F. Chylopericardium in adults: a literature review over the past decade (1996-2006). J Thorac Cardiovasc Surg 2008;136:650-6.
Lewinter M, Imazio M. Pericardial diseases. In: Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF, Braunwald E, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. Elsevier Health Sciences; 2019:1662-80.
Han Z, Li S, Jing H, Liu H. Primary idiopathic chylopericardium: a retrospective case series. BMC Surg 2015;15:61.
Yu X, Jia N, Ye S, Zhou M, Liu D. Primary chylopericardium: a case report and literature review. Exp Ther Med 2018;15:419-25.
Soon SY, Hosmane S, Waterworth P. Chylopericardium after cardiac surgery can be treated successfully by oral dietary manipulation: a case report. J Cardiothorac Surg 2009;4:44.
Marts BC, Naunheim KS, Fiore AC, Pennington DG. Conservative versus surgical management of chylothorax. Am J Surg 1992;164:532-4; discussion 534-5.
Collard JM, Laterre PF, Boemer F, Reynaert M, Ponlot R. Conservative treatment of postsurgical lymphatic leaks with somatostatin-14. Chest 2000;117:902-5.
Szabados E, Toth K, Mezosi E. Use of octreotide in the treatment of chylopericardium. Heart Lung 2011;40:574-5.
Svedjeholm R, Jansson K, Olin C. Primary idiopathic chylopericardium--a case report and review of the literature. Eur J Cardiothorac Surg 1997;11:387-90.
Akamatsu H, Amano J, Sakamoto T, Suzuki A. Primary chylopericardium. Ann Thorac Surg 1994;58:262-6.