Exercise Induced Leg and Calf Pain in an Athlete
A 19-year-old female athlete was referred for exertional leg pain after presenting with deep soleus calf cramping with plantar paresthesia when running on inclines or during repetitive jumping. Her symptoms were significantly worse during the cross-country season. Her medical comorbidities were otherwise unremarkable. Her physical examination revealed reduced pulses in her anterior and posterior tibial arteries with forced plantar flexion bilaterally. Complete blood count, chemistries, lipid, and thyroid stimulating hormone studies were normal. Compartment pressures were measured using the Stryker computer system (Stryker Surgical, Kalamazoo, Michigan) due to claudication symptoms referable to the posterior superficial muscle groups. Resting pressures were measured bilaterally and were normal (<25 mmHg). Non-invasive lower extremity arterial studies were performed and demonstrated normal ankle-brachial indices at rest that decreased to 0.70 and 0.80 during dorsiflexion and plantar flexion bilaterally. Arterial lower extremity ultrasound at the popliteal artery was performed and demonstrated normal triphasic arterial signals at rest with absence of signals during plantar flexion (Figure 1). Magnetic resonance imaging of the lower extremities demonstrated the absence of musculotendinous anomalies.
Figure 1: Arterial lower extremity ultrasound at the left popliteal artery during plantar flexion.
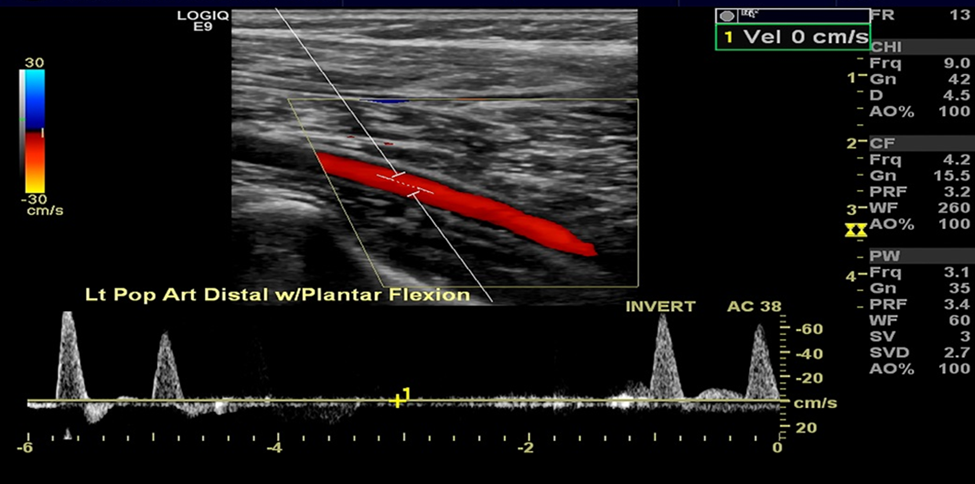
Figure 1
What is the most likely diagnosis of her exertional leg pain?
Show Answer
The correct answer is: D. Functional popliteal artery entrapment syndrome
Exertional leg pain in the athlete may be caused by popliteal artery entrapment, popliteal venous entrapment, external iliac artery endofibrosis, adductor canal compression syndrome, and chronic exertional compartment syndromes (Table 1). Based on the clinical history and physical findings of soleus calf cramping with plantar paresthesia while running, reduced ankle-brachial indices with exertion, absence of Doppler signals during plantar flexion and normal at rest, and normal compartment pressures, functional popliteal artery entrapment was diagnosed. Popliteal artery entrapment syndrome (PAES) is an important cause of exertional leg pain in athletes and is possibly under recognized. Popliteal artery entrapment can be divided into either anatomical and/or functional. Anatomical popliteal artery entrapment syndrome involves the compression of the popliteal artery by surrounding hypertrophied muscle (e.g., medial head of the gastrocnemius, plantaris and soleus muscles) or musculotendinous band and typically causes calf cramping and plantar paresthesia with exertion.1 Functional entrapment occurs with positional compression of the popliteal artery without anatomic abnormalities. Individuals with popliteal venous entrapment can also have similar symptoms that cause venous hypertension and calf swelling and pain with exertion.2 Functional and anatomical PAES are commonly confused with chronic exertional compartment syndrome, as the symptoms often overlap both in quality and location.2-4
Popliteal artery entrapment is a progressive disease from repetitive mechanical compression of the artery that can cause intraluminal stenosis, post-stenotic dilatation and aneurysm formation. This may lead to thrombus formation, embolization, and even ischemia of the lower extremity.2,5 Athletes present with intermittent claudication in the anterior or posterior aspect of the lower extremity. These symptoms typically occur with exertion and may be associated with paresthesia in the tibial nerve distribution and calf swelling. Claudication symptoms have been reported in 50%, digital ischemia in 40% of affected athletes, and paresthesia and calf swelling reported individually in 14% of individuals.6,7 Physical examination should include palpitation of pulses at the dorsalis pedis and posterior tibial with the ankle in passive dorsiflexion and active plantar flexion. Loss of pulse during these maneuvers is diagnostic.
Imaging studies including angiography, computed tomography, and magnetic resonance imaging (MRI) are usually helpful in establishing the diagnosis.8 Diagnostic evaluation also includes noninvasive vascular laboratory testing and imaging. Diagnostic evaluation should include an ankle/brachial index in all athletes with suspected popliteal artery entrapment. The ankle/brachial index are usually within normal limits at rest and abnormal post-exercise.9 Duplex ultrasonography allows for the assessment of blood flow during exacerbating maneuvers.10 Computerized tomography arteriography and magnetic resonance arteriography (MRA) should be performed to evaluate for anatomic popliteal artery entrapment and the surrounding anatomy. Catheter-based angiography remains the gold standard for evaluation of popliteal artery during passive dorsiflexion and active plantar flexion.
Conservative therapy should be tried first, which includes modifying the provoking position with rest, elevation of the lower extremity, and stretching. If symptoms remain after conservative therapy, the mainstay of therapy is surgical compartment release. Popliteal release surgery is performed as a primary procedure if compartment pressures are normal and MRI/MRA studies demonstrate neurovascular compression patterns with functional or anatomic entrapment. Surgical correction in functional popliteal artery entrapment involves fasciotomy of the medial gastrocnemius and mobilization of the soleus attachments to the tibia and fibula. Resection of anomalous muscles is important to relieve anatomic compression on the popliteal artery in anatomic entrapment. If the popliteal artery is severely injured then grafting with placement of a saphenous vein interposition conduit or endarterectomy with a vein patch angioplasty is needed. Success rates close to 100% have been reported for functional and anatomic PAES, with rates between 48% and 57% when the popliteal vein is also entrapped.10 Depending on the type and extent of intervention that is preformed, weight bearing may be limited within the first 4 to 6 weeks postoperatively. Most athletes are back to unrestricted progressive resistance and aerobic conditioning at 6 weeks after surgical intervention.
To conclude, the patient underwent a surgical fasciotomy of the medial gastrocnemius and mobilization of the soleus attachments. The patient recovered well without any post-operative complications and could return to her daily activities 4 weeks following surgery.
Table 1: Differential diagnosis for vascular causes of exertional leg pain
| Diagnosis | History and physical clues | Evaluation/diagnostic tests | Treatment |
| Popliteal artery entrapment syndrome (PAES) |
|
|
|
| External iliac artery endofibrosis |
|
|
|
| Chronic exertional compartment syndrome |
|
|
|
| Cystic adventitial disease |
|
|
|
| Adductor canal compression syndrome |
|
|
|
References
- Grimm NL, Danilkowicz R, Shortell C, Toth AP. Popliteal artery entrapment syndrome. JBJS Rev 2020;8:e0035.
- Shahi N, Arosemena M, Kwon J, Abai B, Salvatore D, DiMuzio P. Functional popliteal artery entrapment syndrome: a review of diagnosis and management. Ann Vasc Surg 2019 Aug;59:259-67.
- Drigny J, Reboursière E, Desvergée A, Ruet A, Hulet C. Concurrent exertional compartment syndrome and functional popliteal artery entrapment syndrome: a case report. PM R 2019;11:669-72.
- Bong MR, Polatsch DB, Jazrawi LM, Rokito AS. Chronic exertional compartment syndrome: diagnosis and management. Bull Hosp Jt Dis 2005;62:77-84.
- Carneiro Júnior FCF, Carrijo ENDA, Araújo ST, Nakano LCU, de Amorim JE, Cacione DG. Popliteal artery entrapment syndrome: a case report and review of the literature. Am J Case Rep 2018;19:29-34.
- Kumar R, Warren P, Mannava K. Popliteal artery entrapment syndrome presenting with critical limb ischemia in an adolescent. J Pediatr 2020;217:215-215.e1.
- Altinsoy HB, Alatas O, Khalil E, Kara KA, Okten CC, Dogan OF. A very rare cause of lower limb ischemia in young people: popliteal artery entrapment. Open Cardiovasc Med J 2018;12:18-28.
- Hai Z, Guangrui S, Yuan Z, et al. CT angiography and MRI in patients with popliteal artery entrapment syndrome. AJR Am J Roentgenol 2008;191:1760-6.
- Levien LJ, Veller MG. Popliteal artery entrapment syndrome: more common than previously recognized. J Vasc Surg 1999;30:587-98.
- Sinha S, Houghton J, Holt PJ, Thompson MM, Loftus IM, Hinchliffe RJ. Popliteal entrapment syndrome. J Vasc Surg 2012;55:252-62.