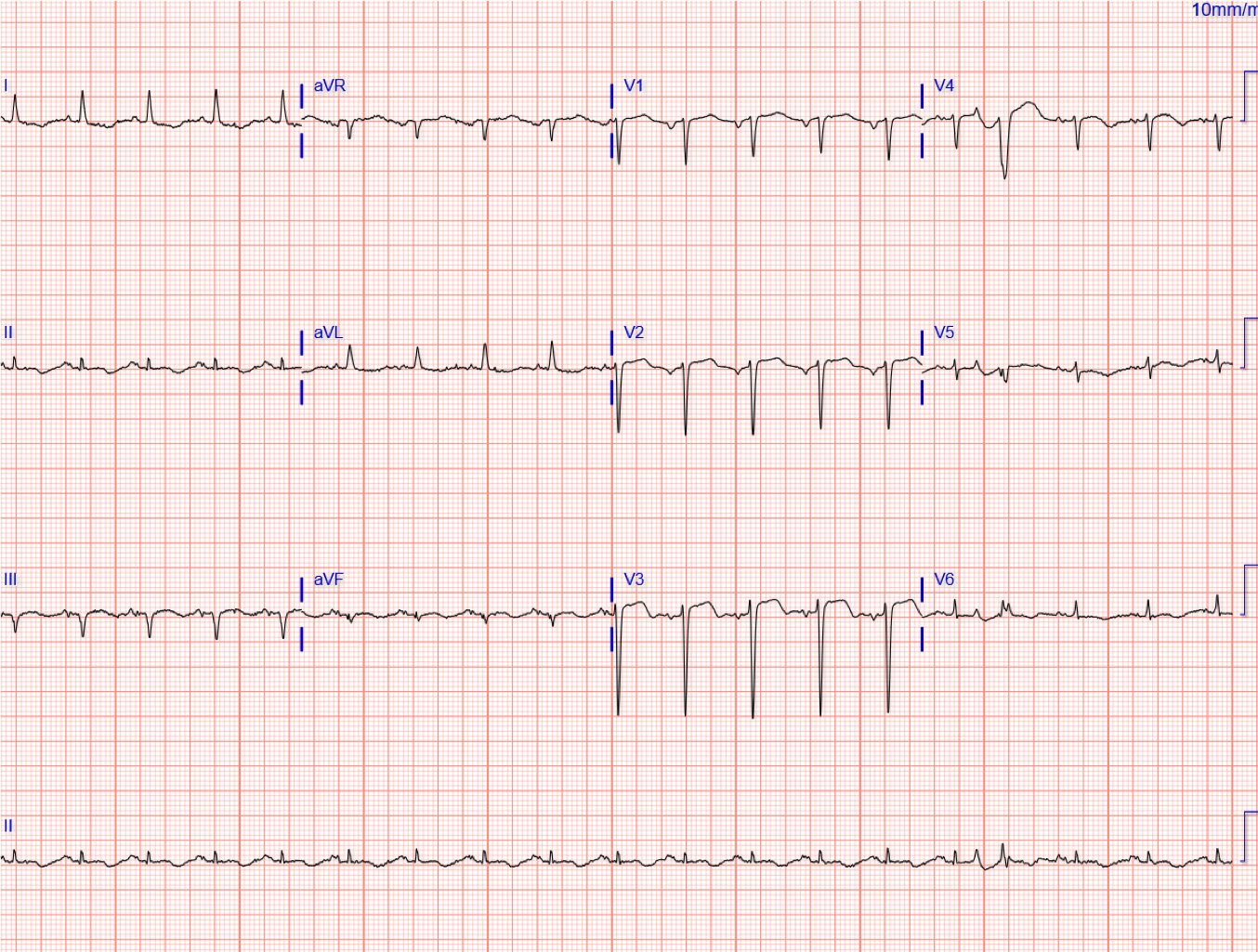
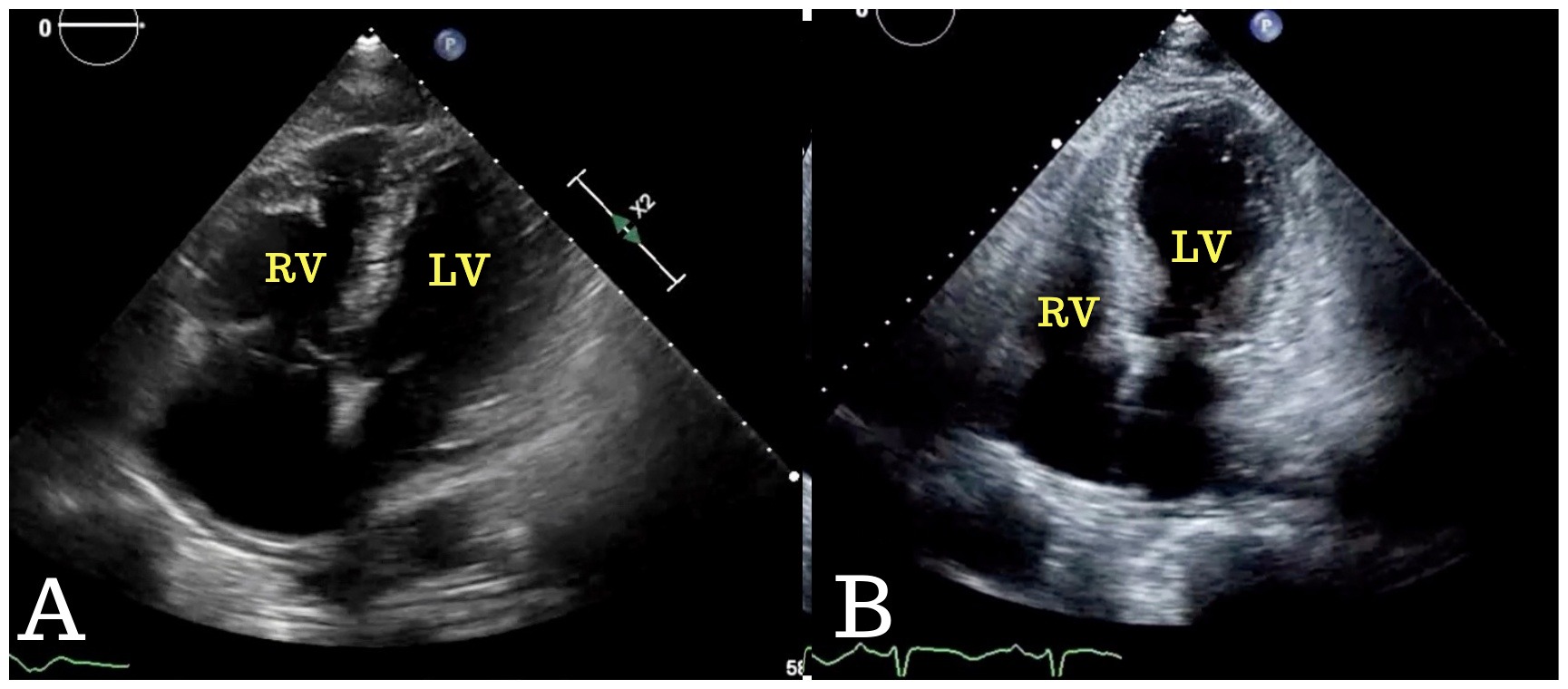
A 74-year-old African American woman presented with troponin leakage and ST-segment elevation in V2-V4 following 12 hours of chest pain (Figure 1). She was transferred to the catheterization laboratory from the emergency department for urgent left-heart catheterization. Coronary angiography showed nonobstructive coronary artery disease, and she was admitted for acute coronary syndrome treatment. She underwent lower extremities venous Doppler that revealed deep venous thrombosis in her right leg. Full-dose heparin infusion was initiated. Transthoracic echocardiography (TTE) was performed on day of admission that showed right ventricular (RV) enlargement and dysfunction with preserved left ventricular (LV) function (Figure 2A, Video 1). Chest computed tomography angiography for ruling out pulmonary embolism was done 2 days after admission and showed bilateral thrombi involving lobar and segmental branches. The Pulmonary Embolism Response Team was activated, and stat TTE was performed per protocol. At this point, TTE showed resolution of RV enlargement and dysfunction. However, acute dilation of apical and mid segments of LV was noted with severe global dysfunction compatible with takotsubo cardiomyopathy (Figure 2B, Video 2). Follow-up TTE in 10 days showed normal RV and LV function (Video 3).
Figure 1
Figure 1
Figure 2
Figure 2
Video 1
Video 1
Video 2
Video 2
Video 3
Video 3
Which of the following statements regarding takotsubo cardiomyopathy is true?
Show Answer
The correct answer is: B. Patients with inverted/basal involvement as opposed to those with classic apical involvement are typically younger and more frequently present with readily discernible physical or emotional triggers.
Takotsubo cardiomyopathy is generally triggered by acute medical illness or intense emotional stress in postmenopausal women. Its typical form is characterized by acute reversible systolic dysfunction of apical and/or mid segments of LV in the absence of obstructive coronary artery disease. Pulmonary thromboembolic events rarely trigger takotsubo cardiomyopathy.1,2 However, several different types of LV and RV involvement have been reported.3 This case is particularly interesting for presenting with acute pulmonary embolism causing RV dilation and dysfunction with resolution of RV failure and emergence of LV dysfunction compatible with takotsubo cardiomyopathy within 48 hours of hospitalization. The prognosis of takotsubo cardiomyopathy is generally favorable, and full recovery of systolic function is expected within a few weeks.4
Although the vast majority of patients with takotsubo cardiomyopathy are women, men have higher risk of in-hospital mortality and major adverse cardiac events.3 Accordingly, answer A is not correct. Because takotsubo cardiomyopathy is not associated with late gadolinium enhancement, cardiac magnetic resonance is valuable for differentiating takotsubo cardiomyopathy from myocardial infarction/myocarditis.5 Accordingly, answer C is not correct. LV function typically recovers within 1-4 weeks; therefore, answer D is not correct.5
References
Jin Q, Luo Q, Zhao Z, et al. Takotsubo syndrome with pulmonary embolism: a case report and literature review. BMC Cardiovasc Disord 2018;18:229. doi:10.1186/s12872-018-0953-7
Baydoun H, Khoueiry G, Ghandour Z, Olkovsky Y. From right to left heart failure: an unexpected transition. Heart Lung 2014;43:41-4.
Dias A, Núñez Gil IJ, Santoro F, et al. Takotsubo syndrome: State-of-the-art review by an expert panel - Part 1. Cardiovasc Revasc Med 2019;20:70-9.
Medina de Chazal H, Del Buono MG, Keyser-Marcus L, et al. Stress Cardiomyopathy Diagnosis and Treatment: JACC State-of-the-Art Review. J Am Coll Cardiol 2018;72:1955-71.
Dias A, Núñez Gil IJ, Santoro F, et al. Takotsubo syndrome: State-of-the-art review by an expert panel - Part 2. Cardiovasc Revasc Med 2019;20:153-66.