A 77-year-old man from Ecuador presents with a 2-month history of progressive fatigue, exertional dyspnea, abdominal distention, and lower extremity edema.
His vital signs were pulse 74, respirations 14 per minute, and blood pressure 102/65 mmHg. Physical examination reveals jugular venous distension that increases with inspiration. The lungs were clear. The cardiac examination reveals soft S1 and S2 with S3 present. The abdomen is distended with a fluid wave. There is 3+ bilateral lower extremity edema to the waist. Laboratory values include CRP 1.8 mg/L and ESR 14 mm/hr. Interferon-gamma release assay for Mycobacterium tuberculosis is positive.
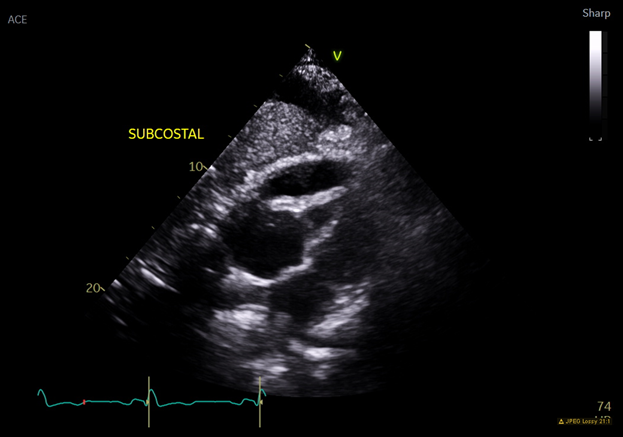
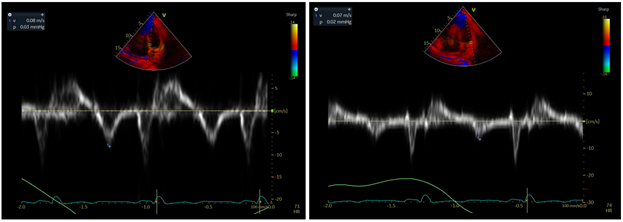
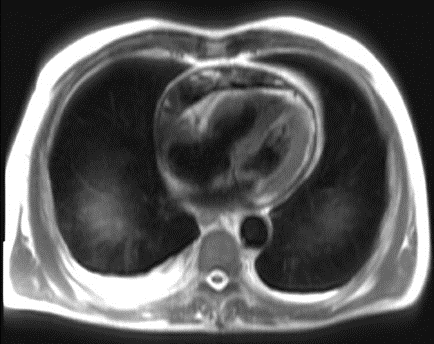
Representative subcostal view and tissue Doppler tracings from his echocardiogram are shown in Figures A and B respectively. Cross sectional imaging from cardiac magnetic resonance imaging (MRI) is shown in Figure C.
Figure A: Transthoracic Echocardiogram
Figure A
Figure B: Tissue Doppler tracings of mitral annulus, medial (left) and lateral (right)
Figure B
Figure C: Cardiac MRI
Figure C
Which of the following would be the most appropriate next step in treatment?
Show Answer
The correct answer is: E. Pericardiectomy
This patient is presenting with signs and symptoms of constrictive pericarditis with elevated jugular venous pressure, ascites, and lower extremity edema. The etiology is most likely chronic tuberculous pericarditis given positive QuantiFERON-TB and living in an endemic region. Tuberculous pericarditis is characterized by insidious onset, and cardiopulmonary complaints are often preceded by fever, night sweats, and weight loss.
Multimodality imaging reveals classic features of constrictive pericarditis. Cardiac MRI demonstrates circumferential pericardial thickening. Echocardiogram reveals a loculated pericardial effusion anterior to the right ventricle and dense pericardial thickening. Tissue Doppler reveals annulus reversus, in which the lateral annulus has less movement than the medial annulus. Normally the lateral annulus has more movement, but there is constraint of the mitral annular motion by the abnormal pericardium with a compensatory increase in the septal motion.1
Definitive treatment involves removal of the diseased pericardium. A biopsy specimen of pericardium should be stained for acid-fast bacilli (AFB) and examined for evidence of granulomatous inflammation.
The addition of corticosteroids to antituberculous therapy may play a role hastening clinical improvement and preventing constriction in patients with tuberculous pericarditis. However, this patient already has constrictive physiology and evidence of chronic disease, thus medical therapy alone is unlikely to alleviate symptoms.2
Pericardial window and pericardiocentesis would not be sufficient to alleviate symptoms.
Use of ibuprofen would not alleviate symptoms; moreover steroids are recommended rather than NSAIDs in the setting of tuberculous pericarditis.
Take Home Points:
Tuberculous pericarditis should be suspected in patients from endemic regions with positive QuantiFERON-TB.
Imaging characteristics of constrictive physiology includes annulus reversus, septal bounce, pericardial thickening and calcification, and pericardial effusion. Clinical signs and symptoms include distended jugular veins with prominent Y descent, pericardial knock, ascites, and lower extremity edema.
Pericardiectomy is the definitive treatment reserved for advanced cases.
References
Alajaji W, Xu B, Sripariwuth A, et al. Noninvasive multimodality imaging for the diagnosis of constrictive pericarditis. Circ Cardiovasc Imaging 2018;11:e007878.
Jung IY, Song YG, Choi JY, et al. Predictive factors for unfavorable outcomes of tuberculous pericarditis in human immunodeficiency virus-uninfected patients in an intermediate tuberculosis burden country. BMC Infect Dis 2016;16:719.