The patient is a 49-year-old African American female with a history of non-ischemic cardiomyopathy with LVEF 30% and multiple admissions for heart failure. Her medications include Entresto 24/26 mg, Metoprolol XL 50 mg BID, and Spironolactone 25 mg BID. Her BP is 96/54, HR 70-80 in AFib, Cr 1.3, and BNP 1047. A parasternal long-axis echo is performed.
Video 1
Video 1
Video 2
Video 2
What is the mechanism of mitral regurgitation?
Show Answer
The correct answer is: B. Functional (secondary) MR
CHOICE A – incorrect - The anterior leaflet never rises above the annulus.
CHOICE C – incorrect - The leaflets open normally in diastole.
CHOICE D – incorrect - The posterior wall motion abnormality and low LVEF excludes this diagnosis.
CHOICE E – incorrect - The anterior leaflet does not prolapse.
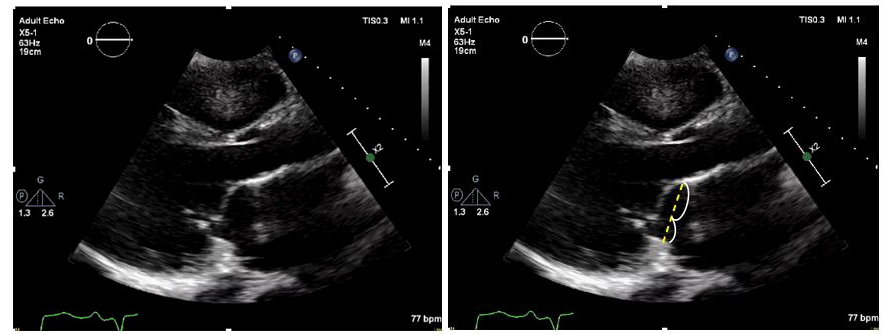
CHOICE B – correct - This is classic functional MR with posterior wall motion abnormality and severe tethering of the posterior leaflet toward the apex. The anterior leaflet is in its normal position but overrides the tethered posterior leaflet. It is not prolapse because in the long-axis view it never moves 2 mm above the annulus.
This is anterior leaflet override, not prolapse.
Anterior Leaflet Override
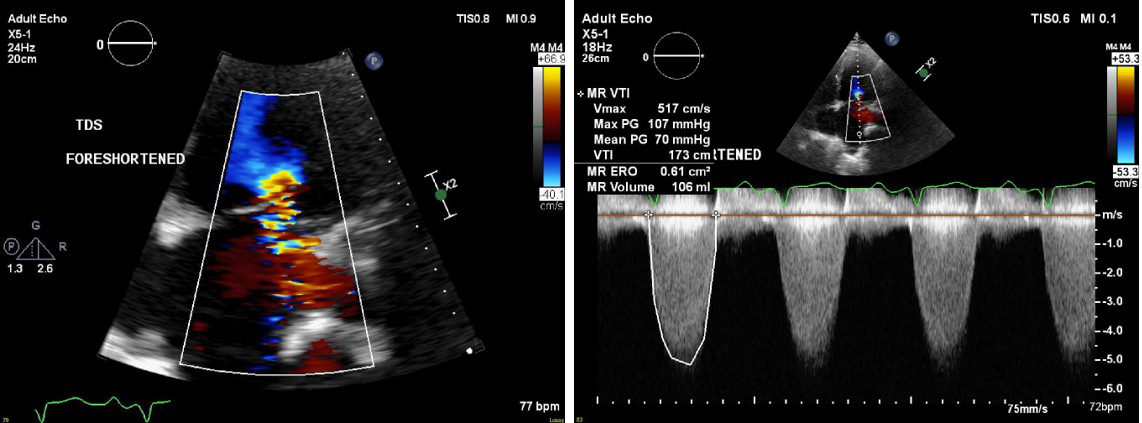
MR Quantitation
MR Quantitation
Optimal treatment of secondary MR
Max tolerated doses of GDMT (forced titration protocols)
CRT when indicated
Coronary revascularization when indicated
Surgical mitral valve repair/replacement currently lack data demonstrating improved survival
COAPT trial showed improved HF hospitalization (primary), mortality and multiple other pre-specified endpoints
Educational grant support provided by Abbott Structural Heart
References
Levine RA, Schwammethal E. Ischemic Mitral Regurgitation on the Threshold of a Solution: From Paradoxes to Unifying Concepts. Circulation 2005;112(5):745-58.
Levine RA, Handschumacher MD, Sanfilippo AJ, et al. Three-dimensional echocardiographic reconstruction of the mitral valve, with implications for the diagnosis of mitral valve prolapse. Circulation 1989;80(3):589-98.