A 34-year-old man is admitted to the hematology ward for severe vomiting and dysphagia, develops severe pleuritic chest pain 4 days after admission.
His medical history is significant for HIV infection diagnosed concurrently with diffuse large B-cell lymphoma (DLBCL) in 2017. He was maintained on Highly Active AntiRetroviral Therapy (HAART) and failed multiple lines of treatment for DLBCL. In that context, he underwent stem cell transplant 48 days prior to assessment. Post-transplant, he developed cutaneous graft versus host disease (GVHD) and was maintained on therapeutic level of immunosuppressive drugs.
Upon admission, the patient was hemodynamically stable but found to be in acute kidney injury thought to be secondary to dehydration. An esophageoduodenoscopy (EGD) was performed to eliminate the possibility of an opportunistic infection explaining his gastrointestinal (GI) symptoms. EGD demonstrated duodenitis but no biopsies were taken as the patient was very agitated throughout the procedure. A repeat EGD was performed 2 days later for biopsies to rule out GVHD.
At the time of assessment, the patient reported a 3-day history of sharp pleuritic chest pain radiating to the back, worsening in the supine position. This pain started 2 days after the first EGD. He denied any associated cough, diaphoresis, palpitations, fever or chills. He did report worsening of longstanding shortness of breath on exertion, present since the stem cell transplant, but denied orthopnea or paroxysmal nocturnal dyspnea.
His resting blood pressure was 116/76 mm Hg with a pulse of 100 beats per minute. He was afebrile and saturating 92% on room air. On exam, he was tachypneic but in no acute distress. There were no distant heart sounds or pericardial friction rub. His jugular veins were not elevated and demonstrated normal variation with respiration. There was no leg edema.
Available laboratory work-up revealed normal electrolytes with a creatinine 154 mmol/L (from 224 mmol/L, normal range 74-107 mmol/L), white blood cell count 4,9 X 109/L, hemoglobin 75 g/L (normal range 120-150 g/L) and platelets 61 X 109/L (at baseline), C-reactive protein 90 mg/L (from 18 mg/L). CD4 count dropped to 48 cells/µL, with CMV PCR negative.
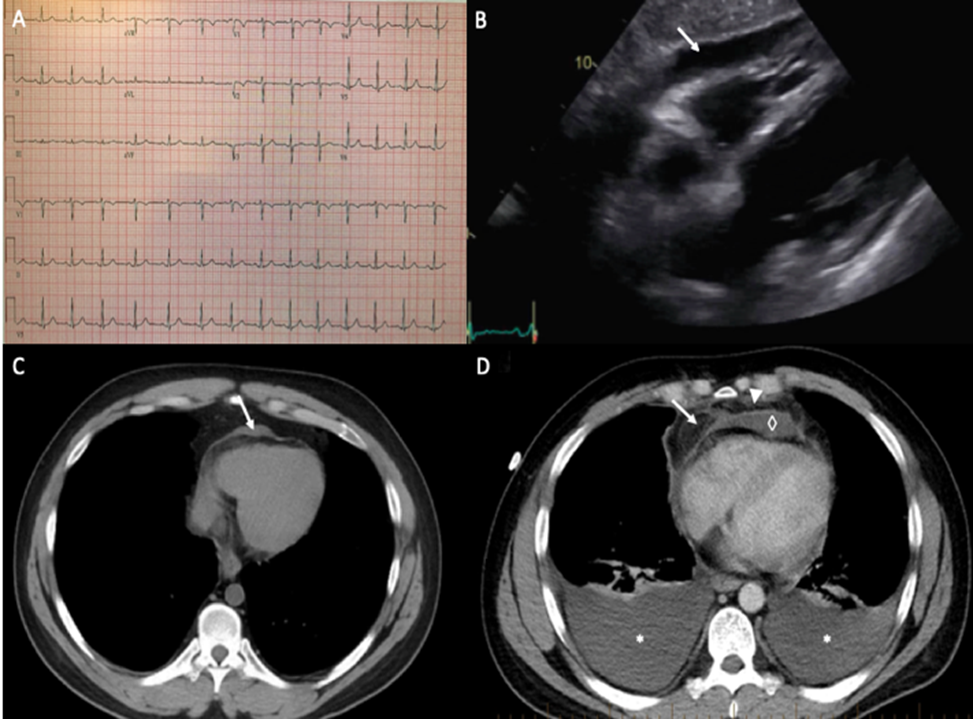
The electrocardiogram (ECG) was unremarkable (Figure 1A).
A transthoracic echocardiogram performed to evaluate his dyspnea and chest pain was significant for a small circumferential pericardial effusion, without chamber collapse, and plethoric IVC suggestive of high right-sided pressures with no frank evidence of tamponade or constrictive physiology (Figure 1B).
A chest computed tomography (CT) scan with contrast was also performed to investigate the patient's dyspnea. It was notable for diffuse pericardial and epicardial fat stranding with mild pericardial collection and enhancement of the pericardium (Figure 1D), highly suspicious for infectious mediastinitis. There was no pneumomediastinum and moderate pleural effusions were noted bilaterally.
Figure 1
Figure 1
Figure 1. A. Patient's ECG showing normal sinus rhythm, without any changes suggestive of pericarditis B. Echocardiography (subcostal view) showing small circumferential pericardial effusion, measured at most 8 mm over the right ventricle. C. Axial chest CT performed 5 months before presentation showing normal pericardium and a small loculated pericardial effusion (arrow). D. Axial chest CT during hospitalization showing thickening of the parietal pericardium (arrow), diffuse pericardial and epicardial fat stranding (arrowhead), bilateral pleural effusion (*), and a small pericardial effusion (◇).
Figure 1. A. Patient's ECG showing normal sinus rhythm, without any changes suggestive of pericarditis B. Echocardiography (subcostal view) showing small circumferential pericardial effusion, measured at most 8 mm over the right ventricle. C. Axial chest CT performed 5 months before presentation showing normal pericardium and a small loculated pericardial effusion (arrow). D. Axial chest CT during hospitalization showing thickening of the parietal pericardium (arrow), diffuse pericardial and epicardial fat stranding (arrowhead), bilateral pleural effusion (*), and a small pericardial effusion (◇).
The possibility of infectious mediastinitis raised the concern for a micro-perforation post-endoscopy given the agitation of the patient during the procedure, but it was judged less likely by the infectious disease specialists. Antibiotics were started nonetheless given the fragility of the patient, and thoracentesis was performed.
Given the new pericardial effusion, typical positional pleuritic chest pain and findings of pericardial fat stranding on CT, the patient was diagnosed with acute pericarditis likely related to contiguous inflammation from the mediastinum.
What would be the most appropriate treatment for this patient's pericarditis?
Show Answer
The correct answer is: C. Prednisone 0.2 mg/kg PO daily + colchicine
With regards to pericarditis, the first line of treatment normally consists of high-dose aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs). However, many conditions preclude the use of NSAIDs and aspirin, including bleeding risk (e.g. thrombocytopenia), renal failure, peptic ulcer disease, all of which our patient had. Corticosteroids are usually second-line treatment for pericarditis in patients who have contra-indications to receiving anti-inflammatories, as they can prolong the course of disease. Antimicrobial therapy is warranted for the treatment of purulent pericarditis, but watchful waiting with antibiotics only was not the right answer since the patient had severe chest pain significantly limiting his quality of life, and we wanted to avoid the risk of developing constrictive/effusive-constrictive pericarditis.
The patient's symptoms improved significantly on low dose prednisone over a week and CRP markedly improved. All cultures came back negative and antibiotics were stopped. Unfortunately, the pleural fluid analysis was consistent with recurrence of malignancy. The patient was subsequently started on rituximab and high dose prednisone was continued as a part of the chemotherapy treatment of DLBCL.
The patient's clinical history, features and imaging findings are consistent with both mediastinitis and pericarditis. Most cases of pericarditis are deemed to be idiopathic or post-viral. Rarely, a specific infectious pathogen is identified such as Mycobacterium tuberculosis and Borrelia burgdorferi. Pericarditis can also be seen after a variety of cardiac procedures from simple pacemaker insertion to cardiac surgery. Rarer causes of pericarditis include Dressler's syndrome, autoimmune diseases, malignancy, hypothyroidism, and radiation.1 More recently, checkpoint inhibitors have been identified as a cause of immune-mediated myocarditis and pericarditis.2
Mediastinitis is somewhat of a rare clinical instance and nowadays is most often seen after cardiac or thoracic surgery. Occasionally, it can develop from esophageal perforation (iatrogenic after gastroscopy or from foreign body ingestion), from contiguous spread of odontogenic or retropharyngeal infections (pharyngitis, tonsillitis, peritonsillar abscess), from penetrating trauma to the chest or from hematogenous spread.3 Mediastinitis usually presents with fever, chest pain, sternal instability and signs of sternal wound infection, typically 2 weeks after cardiac surgery. The diagnosis is clinical but can be supported by CT which shows localized mediastinal fluid, fat stranding and pneumomediastinum.4 The treatment involves prolonged antibiotics course and usually surgical debridement.
Although rare, there have been reports of mediastinal disease spreading to the pericardium, or vice versa, which can be explained by the continuity and contiguity between both structures.5 Given that the pericardium is a fixed, enclosed space, infections in this setting are treated as abscesses with drainage for infectious source control, and to prevent development of pericardial fibrosis which could lead to constrictive physiology.
The role of multimodality imaging in complex pericardial disease is more and more recognized. Imaging the pericardium by echocardiography can be challenging, yet it remains the first line in pericardial disease. It is widely available, cost effective and does not require any radiation. It also provides hemodynamic data in case of constriction, but it lacks sensitivity to detect pericardial thickening in mild pericarditis.6
Cardiac-gated computed tomography (CCT) or cardiac magnetic resonance imaging are both second line modalities to interrogate the pericardium. The high spatial resolution of CCT makes it the most accurate modality to detect pericardial thickness (>2.0 mm).7 Despite a rapid and accurate acquisition, the need for iodinated contrast, radiation and the lack of hemodynamic information preclude a more widespread use of this modality.
Signs of acute pericarditis on CCT include thickened smooth pericardium and pericardial effusion. Also, iodinated contrast enhancement represents ongoing inflammation either on visceral or parietal surfaces.8 As the duration of the inflammation increases, the pericardium can develop irregular contours. Nodularity of the pericardium can also suggest metastatic disease in patients known with neoplasia.9 Characterization of the pericardial effusion is also possible with this modality. Exudative effusion will typically show an attenuation measurement >25 HU, which can be seen in hemopericardium, malignancy purulent exudates and effusions related to hypothyroidism.10 Furthermore, it is also the most sensitive imaging modality to detect pericardial calcification in constrictive pericarditis.11 CCT is not recommended to evaluate for acute tamponade.
In summary, pericardial diseases are challenging to diagnose and can be overlooked in that context. Untreated disease can result in important morbidities for the patient. This case shows the importance of reviewing all the images available, as a CT scan performed for another indication can provide relevant information to the clinician about the pericardium. As the echocardiography remains the first line, cardiac CT can provide additional information regarding to the etiology of the inflammation and its extension to the surrounding tissues.
References
Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA 2015;314:1498-506.
Hu JR, Florido R, Lipson EJ, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc Res 2019;115:854-68.
Inaco Cirino LM, Melhem Elias F, Jesus de Almeida JL. Descending mediastinitis: a review. Sao Paulo Med J 2006;124:285-90.
Exarhos DN, Malagari K, Tsatalou EG, et al. Acute mediastinitis: spectrum of computed tomography findings. Eur Radiol 2005;15:1569-74.
Man MA, NiTu MF, Strambu L, Florescu C, Streba CT, Trofor AC. Tuberculous constrictive pericarditis complicated with tuberculous mediastinitis - case report. Rom J Morphol Embryol 2016;57:237-42.
Al-Mallah MH, Almasoudi F, Ebid M, Ahmed AM, Jamiel A. Multimodality imaging of pericardial diseases. Curr Treat Options Cardiovasc Med 2017;19:89.
Kligerman S. Imaging of pericardial disease. Radiol Clin North Am 2019;57:179-99.
Chetrit M, Xu B, Kwon DH, et al. Imaging-guided therapies for pericardial diseases. JACC Cardiovasc Imaging 2020;13:1422-37.
Chetrit M, Xu B, Verma BR, Klein AL. Multimodality imaging for the assessment of pericardial diseases. Curr Cardiol Rep 2019;21:41.
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Klein AL, Abbara S, Agler DA, et al. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr 2013;26:965-1012.e15.