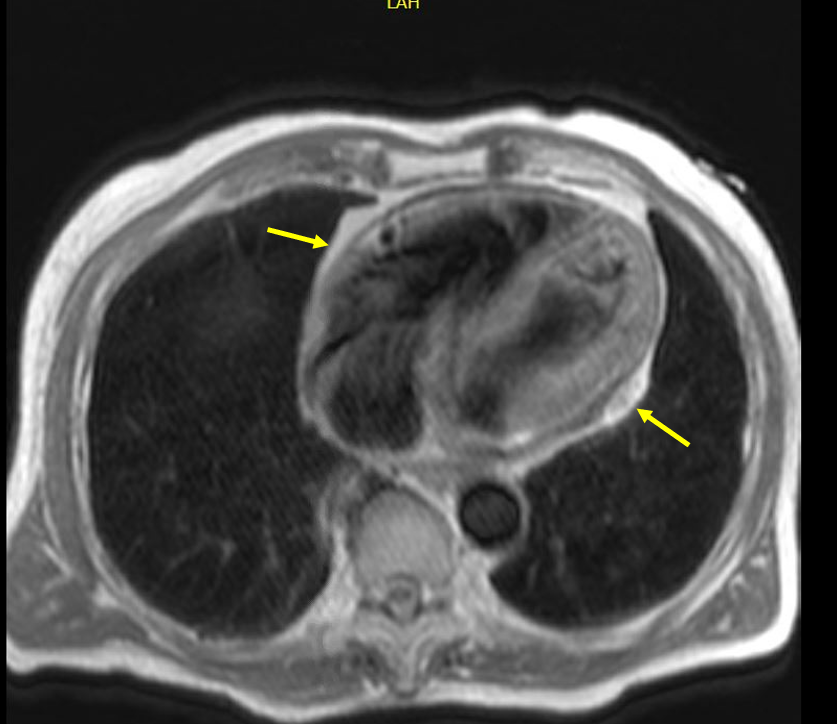
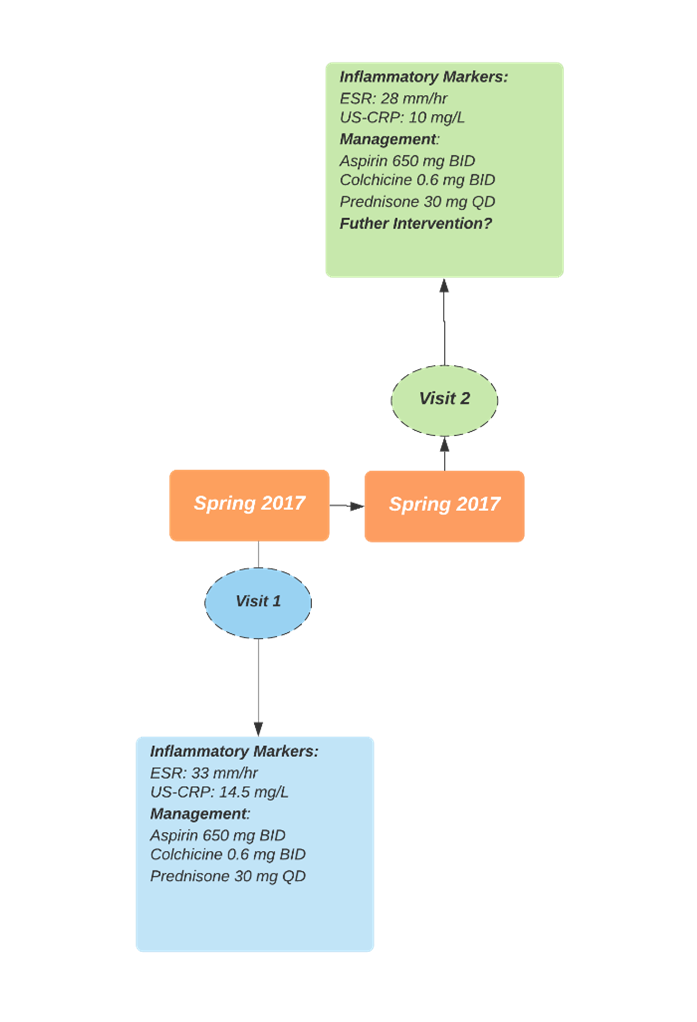
A 79-year-old male with history of insulin dependent diabetes mellitus, paroxysmal atrial fibrillation on apixaban and hyperlipidemia presented to the emergency department (ED) for dyspnea on exertion, transient chest pain, worsening lower extremity edema and weight gain of 20 pounds over a week prior to presentation. He underwent echocardiography (ECHO) which demonstrated 45% ejection fraction and revealed a small pericardial effusion. He underwent diuresis with torsemide 20 mg once daily, started on metoprolol succinate 25 mg once daily and discharged home with cardiology follow up after resolution of symptoms. At cardiology clinic, he was found to have elevated erythrocyte sedimentation rate (ESR) Westergren 33 mm/hour (reference range: 0-15 mm/hour) and ultra-sensitive C-reactive protein (US-CRP) 14.5 mg/L (reference range: <3.1 mg/L) and he was started on aspirin, colchicine, and prednisone for pericarditis. A month later, he was admitted again for lower extremity edema. Comprehensive physical examination revealed jugular venous distension to 17 cm, ascites, pericardial knock, and lower extremity swelling bilaterally. He was started on intravenous furosemide for diuresis. Apixaban was held due to high risk of bleeding in the presence of active pericarditis. He underwent cardiac catheterization which showed mild coronary artery disease. Cardiac magnetic resonance imaging (CMR) was also obtained which revealed diffuse pericardial thickening (4 mm) (Figure 1) and enhancement, moderate-sized circumferential pericardial effusion, and a prominent septal bounce with abnormal early diastolic motion of the interventricular septum. Delayed enhancement imaging demonstrated enhancement of both visceral and parietal layers, all in keeping with an inflammatory, effusive pericarditis. The inflammatory markers were obtained which were elevated ESR 28 mm/hour and US-CRP 10 mg/L. ECHO was obtained again which demonstrated 42% ejection fraction, prominent septal bounce, circumferential pericardial thickening, and small right sided pericardial effusion. The right/left ventricle apex, right atrium and lateral wall of the left ventricle appeared to be tethered. Inferior vena cava was dilated with <50% collapse. There was annulus reversus and significant respiratory variation across the mitral/tricuspid valve suggestive of constrictive physiology. Patient did not have any personal history of autoimmune conditions, tuberculosis, chest radiation, any viral illness in the past or trauma. The treatment timeline is given in Figure 2.
Figure 2. Treatment timeline of the patient up until the intervention.
Figure 2. Treatment timeline of the patient up until the intervention.
What is the next course of management?
Show Answer
The correct answer is: C. Initiate anakinra alongside triple therapy with aspirin, colchicine, and prednisone
Constrictive pericarditis has traditionally been treated by surgical intervention. Although surgery is definitive, it carries additional risks for certain patient populations and is far more invasive than medical management. Pharmacologic management is often involved in the treatment of constrictive pericarditis. These agents play a role in acute symptom relief, decreasing overall symptom burden, and the prevention of progression to chronic pericardial constriction. In cases of transient constrictive pericarditis, oral anti-inflammatory drugs are the initial choice due to their ability to decrease pericardial inflammation, reverse the development of constrictive physiology, and reduce recurrence of acute pericarditis.1 Clinical and laboratory tools such as inflammatory markers can help identify patients that would benefit from anti-inflammatory therapy. ESR and CRP are useful markers of inflammation that can help direct treatment decisions. CMR is an integral part of the diagnosis because it can differentiate active pericardial inflammation from chronic inflammation involving fibrosis. Specifically, greater degrees of gadolinium enhancement on qualitative assessment appear to have better responses to anti-inflammatory therapy in the treatment of constrictive pericarditis.2 In terms of anti-inflammatory drugs, non-steroidal anti-inflammatory drugs (NSAID) and colchicine are typically the drugs of choice as evidenced by their effects in reducing acute inflammation and limiting recurrence of pericarditis.1 Oral corticosteroid therapy is another anti-inflammatory that is successful in treating transient constrictive pericarditis, more commonly implemented for refractory cases or for individuals with contraindications to NSAIDs or colchicine.1 However, steroids are used with caution in pericarditis due to the risk of systemic effects as well as recurrence of disease if steroid therapy is implemented early in the disease course at high doses.1 If the response to therapy is suboptimal with NSAID and colchicine, or steroids, triple therapy with all three agents can be implemented.3
Newer agents have been described as alternative therapy for the treatment of constrictive pericarditis in the literature. These agents are alternatives to traditional medical therapy or used in cases where a patient develops corticosteroid-dependent pericarditis or colchicine-resistant pericarditis.3 For patients with signs of systemic inflammation, anakinra, a nonselective interleukin-1 receptor antagonist, is recommended.3 Evidence about the use of these agents is limited to case reports and case series, however, anakinra use in cases of refractory pericarditis has shown benefit in a preliminary study by reducing pericarditis flares and the risk of recurrence.4 The dose of anakinra for transient constrictive pericarditis is 1-2 mg/kg/day with a maximum dose of 100 mg/day.1
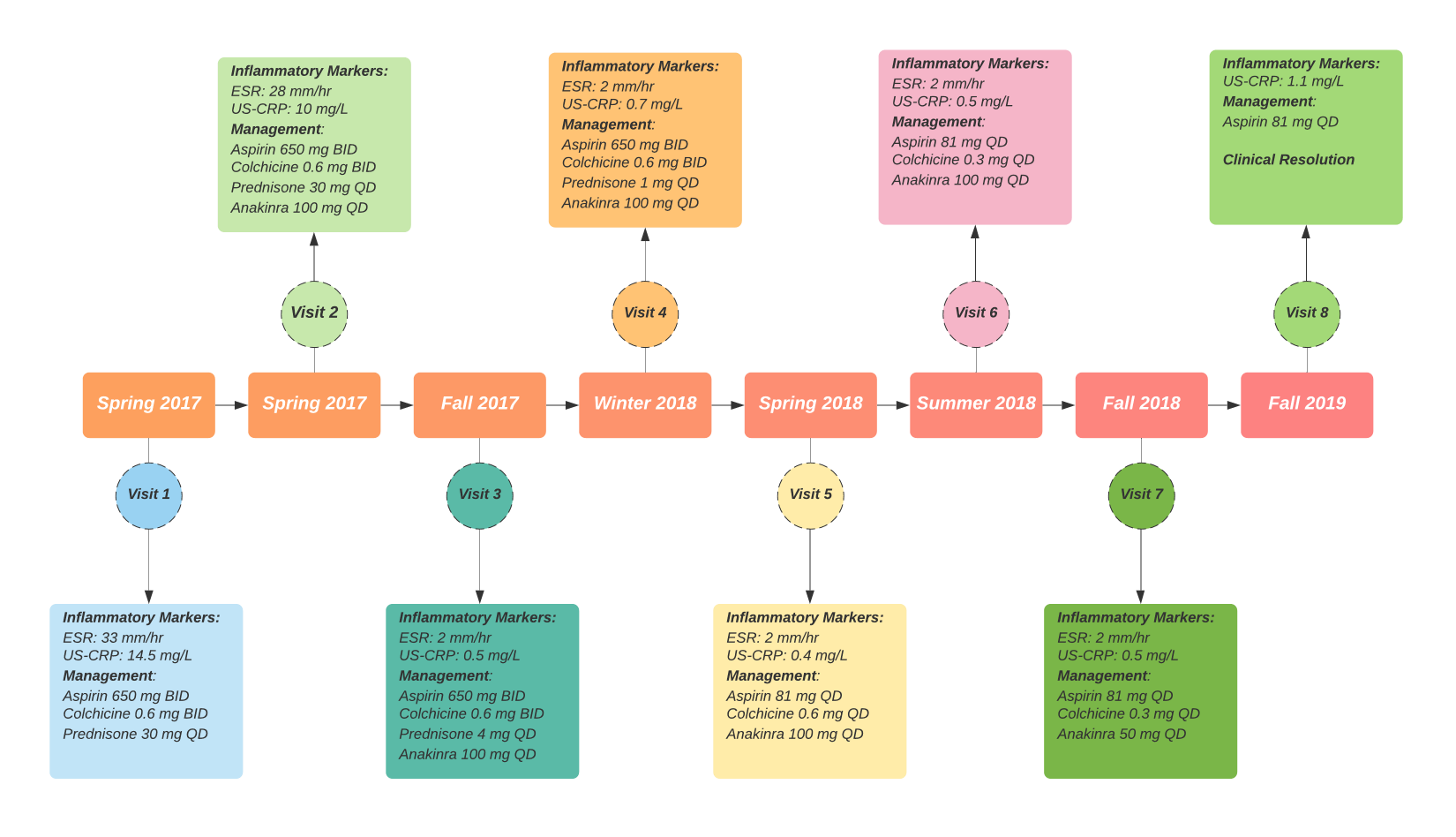
Our patient was diagnosed with transient effusive constrictive pericarditis. He was never started on any anti-inflammatory therapy prior. During hospitalization, rheumatology was also consulted, and it was decided to initiate anakinra 100 mg subcutaneously daily along with the triple therapy (aspirin 650 mg twice daily, colchicine 0.6 mg twice daily and prednisone 30 mg once daily with slow taper). He was discharged on this quadruple regimen with follow up at our pericardial clinic. Patient reported no symptoms and normalization of inflammatory markers was witnessed. We were able to wean him off the prednisone by slow taper. Repeat CMR was obtained after 6 months which showed reduction in the amount of pericardial effusion, degree of delayed pericardial enhancement, circumferential pericardial thickening, and septal bounce. He no longer had recurrence of pericarditis. The entire treatment timeline is illustrated in Figure 3.
Figure 3
Figure 3
Figure 3. The detailed treatment timeline of the patient.
Figure 3. The detailed treatment timeline of the patient.
References
Gentry J, Klein AL, Jellis CL. Transient constrictive pericarditis: current diagnostic and therapeutic strategies. Curr Cardiol Rep 2016;18:41.
Miranda WR, Oh JK. Constrictive pericarditis: a practical clinical approach, Prog Cardiovasc Dis 2017;59:369-79.
Imazio M. Noninfectious pericarditis: management challenges for cardiologists. Kardiol Pol 2020;78:396-403.
Brucato A, Imazio M, Gattorno M, et al. Effect of anakinra on recurrent pericarditis among patients with colchicine resistance and corticosteroid dependence: the AIRTRIP randomized clinical trial. JAMA 2016;316:1906–12.